







| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Original Article
Volume 3, Number 1, February 2014, pages 8-13
E-mail Communication in the OB/GYN Office: Analysis of Patient E-mails to Their OB/GYN
Andrew L. Atkinsona, b, Jonathan D. Bauma, Meghan Rattigana, Debra Gussmana
aDepartment of Obstetrics and Gynecology, Jersey Shore University Medical Center, Neptune, NJ, USA
bCorresponding author: Andrew Atkinson, Department of Obstetrics and Gynecology, Jersey Shore University Medical Center, 1945 State Route 33, Neptune, NJ 07754, USA
Manuscript accepted for publication January 10, 2014
Short title: E-mail Communication From Patients
doi: https://doi.org/10.14740/jcgo232e
| Abstract | ▴Top |
Background: How patients use e-mail with their obstetrician-gynecologists (ob/gyns) is unknown. E-mail was originally created as a tool for health care professionals yet physicians remain reluctant to adopt e-mail as a form of communication with patients. Many cite concerns of patient misuse, risk management issues, and uncompensated time commitment. The primary objective of this study was to examine the details of e-mail generated by patients to their ob/gyns. A secondary objective was to examine e-mails that corroborate physician concern about e-mail.
Methods: A retrospective observational study was performed. E-mails from patients sent to two ob/gyns were examined.
Results: Three hundred patient initiated e-mails were generated by 127 patients. Seventy-eight percent were sent during office hours and 87% of e-mails were sent on weekdays. Thirty-seven percent involved symptoms, 14% test results, 13% administrative, 12% contraception, 11% prescriptions, 8% other and 5% social. Three percent of e-mails met the definition of misuse. There were 594 follow-up e-mails exchanged from the initial 300 e-mails. Each physician received up to 6 e-mails daily.
Conclusions: Patients use e-mail as an alternative to calling. More than 50% of e-mails relate to symptoms and test results. This study substantiated concerns about e-mail misuse by patients. New policies must be created to ensure that e-mail with patients is safe, effective and attractive for physicians as a form of communication with patients.
Keywords: E-mail; Electronic mail; Physician communication; OB/GYN
| Introduction | ▴Top |
In 2000, the American Medical Association (AMA) endorsed e-mail and developed guidelines for e-mailing with patients [1, 2]. Brooks (2006) reported that 85% of physicians had high speed internet access yet only 16.6% of them used e-mail with patients based on a survey of 4,203 primary care physicians [3]. Boukus (2010) reported only 6.7 percent of office based physicians routinely e-mailed their patients [4]. A 2012 Wall Street Journal article reported that 40% of physicians e-mailed patients [5]. The California HealthCare Foundation (2010) reported that 70% of adults wanted to use e-mail to communicate with their health care providers [6].
There are 3.6 billion e-mail accounts in existence with approximately 2.7 billion users worldwide [7]. An estimated 155 billion e-mails are sent each day with an average of 2.8 million messages sent per second [7]. The first electronic mail was sent in 1971 [8]. The word “e-mail” was coined in 1982, when the United States Copyright office awarded copyright to a precocious 14-year-old for the development of an “electronified” version of a paper mail system [8]. The main drive behind this creation was to enable physicians to distribute information across campuses at the University of Medicine and Dentistry of New Jersey [8]. The birth of an electronic form of communication was motivated to ease communication barriers experienced by health care professionals at that time [9].
Although e-mail was originally created as a tool for healthcare professionals, physicians remain reluctant to use e-mail with patients. There is fear of misuse, including liability, privacy breaches, software/hardware malfunction and uncompensated time commitment [10, 11].
There is a paucity of reports regarding e-mail use with patients. A PUBMED search was conducted using the terms “electronic mail”, “e-mail”, “email” and “physician communication” to identify studies about physician use of e-mail. Only three reports examined e-mail communication between physicians and patients in the private practice setting [11-13]. Sittig (2003) analyzed e-mail content and characteristics of communication between internists and their patients [11]. White (2004) looked at patient and provider e-mail in a private family practice setting and Anand (2005) looked at e-mail between providers and parents in a pediatric practice [12, 13]. There were no studies examining e-mail between obstetrician-gynecologists (ob/gyns) and their patients. The American College of Obstetricians and Gynecologists mentions e-mail in two Committee Opinions as an alternate method of communication [14, 15]. Electronic records and electronic communication are prominent features of the Affordable Care Act of 2010 which makes e-mail relevant in a modern healthcare system [16].
The primary objective of this study was to examine the details of e-mail initiated by patients to their ob/gyns. A secondary objective was to corroborate physician concerns about e-mail.
| Materials and Methods | ▴Top |
An Institutional Review Board (IRB) approved this retrospective observational study. Three hundred patient initiated e-mails sent to a suburban ob/gyn practice were examined over two non-consecutive three-month blocks for a total collection time of six months. Physicians instructed all interested patients on the proper use and availability of e-mail. Each patient was given a handout that was based on AMA, American Medical Informatics Association (AMIA) guidelines, as well as institutional policies on e-mail [1, 2, 17]. Patients were told to expect a response within 48 hours of receipt and advised to avoid e-mailing in regard to any medical emergencies. They were instructed to call the office if there was no response to their e-mails. Physicians would personally respond to e-mails regarding test results, symptoms and prescriptions. All e-mail exchanges by physicians were encrypted in accordance with privacy policies.
E-mails were examined for time of day, day of the week received, and content. Information about date, time, and day of the week were obtained from each physician’s inbox. E-mails were read and grouped by theme. Seven categories emerged: symptoms, test results, administrative, contraception, prescriptions, social and other. Each e-mail was assigned to one category (Table 1). If more than one topic was discussed in an e-mail, the category assignment was made based on word count. Each e-mail was examined to determine if it required physician knowledge to be properly answered.
 Click to view | Table 1. E-mail Content by Category |
E-mail was examined for misuse, including liability and privacy breaches. We defined email misuse as inappropriate content including medical emergencies, unclear or confusing format, failure to use sender’s full name, length greater than 250 words, or more than one e-mail per month. Privacy was measured by e-mails that did not comply with AMA, AMIA, or institutional guidelines. E-mail was also examined for malware, spyware and viruses. The number of times that physicians responded was recorded.
| Results | ▴Top |
Three hundred patient initiated e-mails were generated by 127 patients. There were 297 available for analysis, three were excluded because they could not be opened. We calculated the number of emails per physician per day by looking at the number of unread email’s in each physician’s inbox during business hours. All e-mails were in English. A total of 121 (41%) e-mails were sent by obstetric patients, 125 (42%) were sent by gynecologic patients and 51 (17%) could not be identified as either by e-mail content.
Two hundred thirty-four (78%) e-mails were sent during office hours of 8:00 AM and 6:00 PM (Fig. 1). Two hundred sixty-two (88%) e-mails were sent on weekdays (Fig. 2). Monday was the busiest day for e-mails, 64 (21%). The average number of e-mails reviewed by each physician was 3 per day during business hours. Distribution of e-mail content by category can be found in Figure 3. A physician’s response was required in 144 (48%).
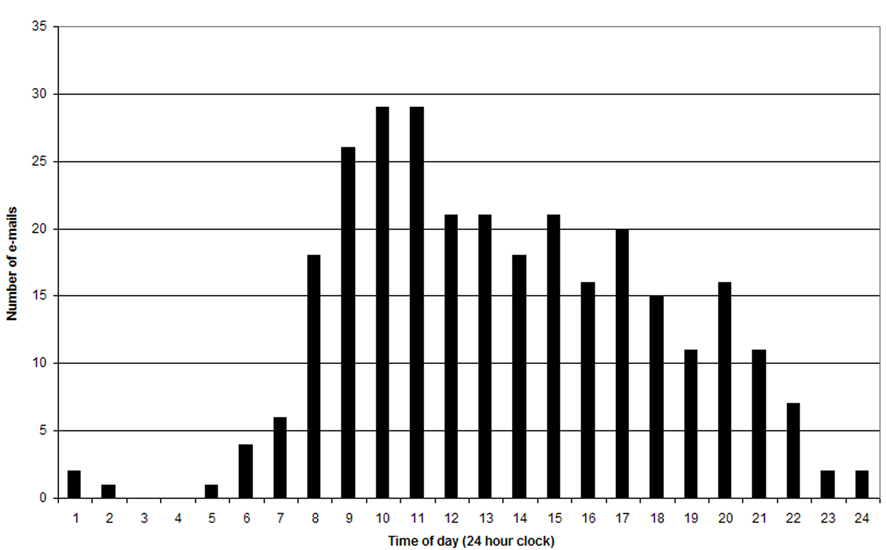 Click for large image | Figure 1. E-mails sent by hour of day. |
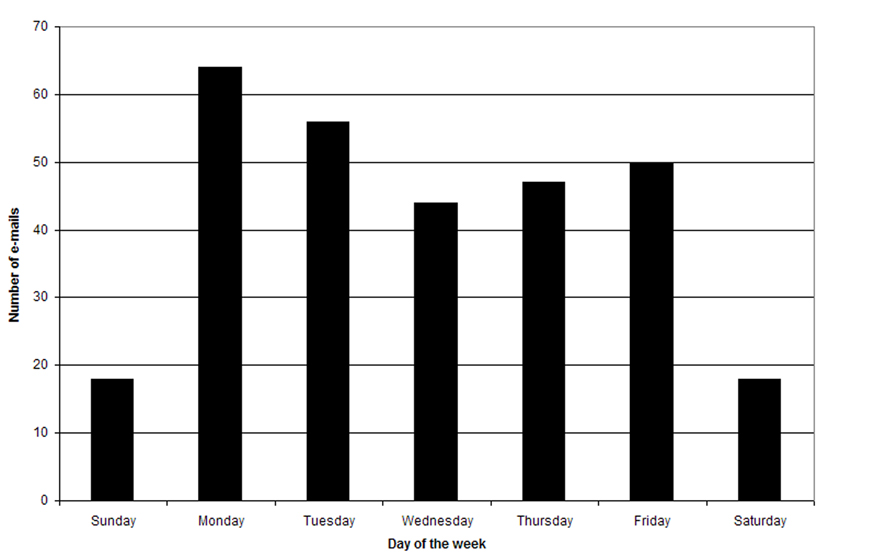 Click for large image | Figure 2. E-mails sent by day of the week. |
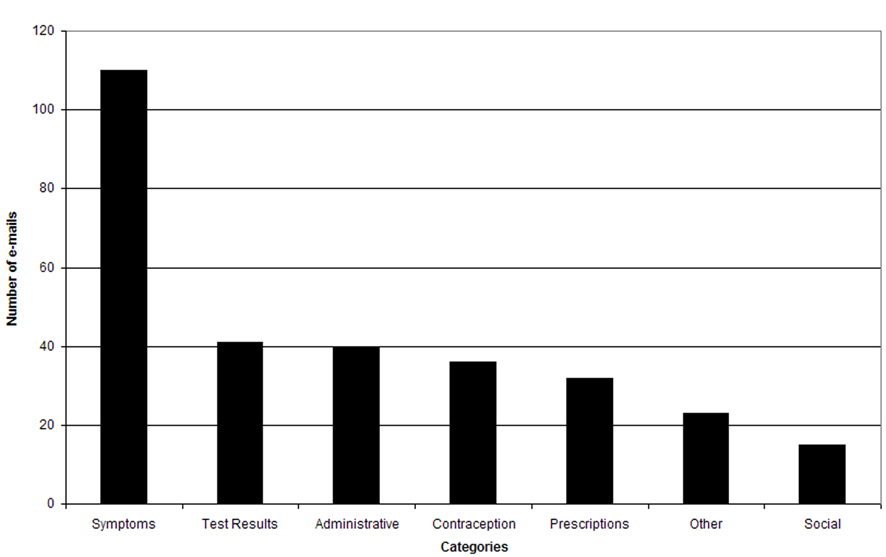 Click for large image | Figure 3. E-mail content. |
There were examples of misuse in eight (2.7%) e-mails. Three were sent by obstetric patients, two from gynecologic patients, and three could not be opened. Two pregnant patients wrote about “contractions”, one at 30 weeks and the other at unknown gestational age. Another pregnant patient wrote about severe abdominal pain and signed her e-mail with her first name only. A gynecologic patient wrote “Right arm tingle, right leg feels different too Shiould I take an aspirin? [sic]”. Another gynecologic patient wrote about facial hives that occurred after taking an unspecified medication. No known privacy breaches, malware/spyware, or viruses were observed.
There were 594 follow-up e-mails exchanged from the initial 300 e-mails. A physician provided a single response in 157 (53%) e-mails, two responses in 67 (23%), and three or more e-mail responses in 73 (25%) of patient initiated e-mails. One e-mail required eight responses.
| Discussion | ▴Top |
We began this study to examine the details of e-mails generated by patients to their ob-gyn. A secondary objective was to investigate e-mail qualities that substantiate physician reluctance to use e-mail to communicate with patients.
In this study, both obstetric and gynecologic patients initiated e-mail. The majority of e-mails were sent when the office was open and staff was available to answer the telephone. This is evidence that there are patients who prefer to e-mail rather than use the telephone as a means to communicate with their physician.
Three percent of e-mails met the definition of misuse despite physician instruction on proper use. Emergency conditions such as potential stroke, anaphylaxis, abruption, and preterm labor were communicated via e-mail. Emergencies are not appropriate topics for e-mail since the time when an e-mail message will be read and acted upon cannot be ascertained [17]. Delay may lead to harm and increased liability. If e-mail is to be used by a practice, the practice must assume the burden of educating patients and policing incoming e-mail for misuse.
Participating physicians readily recalled prior anecdotes of patient misuse worth noting. One patient e-mailed 109 times during a pregnancy. Another patient e-mailed 60 times over the course of a year regarding menopause. Another example of inappropriate use involved a patient and her mother who conducted an acrimonious conflict using e-mail, putting the physician in the middle of their quarrel.
Many patients e-mailed about symptoms. Approximately half of the e-mails required a physician’s attention. A similar observation has been made by others. Sittig (2003) analyzed e-mail content and found that 48% required a physician’s response [11]. White (2004) reported that 43% of e-mails required a physician’s response [12]. Anand (2005) found 53% required a physician’s response [13]. Since approximately half of e-mails do not require a physician attention and there is the potential for misuse, e-mail cannot be the sole responsibility of non-professional administrative staff. A system of triage must be used. Clinical questions must be answered in a suitable time period and e-mails with emergency content warrant an immediate response. It is reassuring that three of the five patients with potential emergencies had their issues addressed promptly via e-mail as they occurred during business hours. However, it is concerning that the other two potential emergencies were not addressed in a timely fashion. Most practices have a telephone policy to avoid a delay in triage. Similar policies must be developed for e-mail.
Physicians received patient initiated e-mails on most days. About half of e-mails required multiple responses. Time commitment for responses to patient e-mail is unknown. However Baron (2010) reported that the average primary care physician engages in 24 phone calls daily with a time commitment of 60 minutes [18]. It is not known if e-mail can reduce the burden of phone calls or if it only adds an additional burden for the physician. The time commitment for e-mail needs further study.
Privacy is a potential problem in any communication system. Phone conversations may be overheard or misdirected especially with voicemail. Written materials may be misplaced or left exposed to public view. E-mails may be mishandled, sent or forwarded to the wrong recipient. While privacy rules apply in all patient/physician interactions, it is worth noting that e-mail privacy may not be guaranteed despite encryption technology.
In this paper, we report how our patients used e-mail. Approximately half of e-mails received required the attention of a physician. Several examples of e-mail misuse were noted and physician concern is warranted. It has been more than 13 years since the AMA endorsed e-mail with patients yet adoption rates by physicians remain low. New policies must be created to ensure that e-mail with patients is safe, effective and attractive for physicians as a form of communication with patients. The impact of patient e-mail in regard to uncompensated time commitment needs further study.
Acknowledgments
The authors would like to thank Andrew Blechman, MD for his help in editing this manuscript.
Financial Disclosure
No financial gain or funding was used or obtained for this study.
Conflicts of Interest
The authors of this manuscript have no conflicts of interest to report.
| References | ▴Top |
- Goldschmidt D. AMA passes guidelines for doctor/patient e-mail. Available at http://archives.cnn.com/2000/HEALTH/06/14/medical.email/index.html. Retrieved June 16, 2013.
- Opinion 5.026. The use of electronic mail. American Medical Association. Available at http://www.ama-assn.org//ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion5026.page Retrieved on October 29, 2013.
- Brooks RG, Menachemi N. Physicians' use of email with patients: factors influencing electronic communication and adherence to best practices. J Med Internet Res. 2006;8(1):e2.
doi pubmed - Boukus ER, Grossman JM, O'Malley AS. Physicians slow to e-mail routinely with patients. Issue Brief Cent Stud Health Syst Change. 2010;(134):1-5.
- Kvedar JC, Bierstock S. Should physicians use email to communicate with patients? Wall Street Journal. January 23, 2012.
- California HealthCare Foundation. (2010). Consumers and Health Information Technology: A National Survey. Available at http://www.chcf.org/publications/2010/04/consumers-and-health-information-technology-a-national-survey Retrieved on October 28, 2013.
- Radicati S, Hoang Q. Email Statistics Report, 2012-2016. Available at: http://www.radicati.com/?p=8262/ Retrieved on October 29, 2013.
- Aamoth D. The man who invented email. Available at: http://techland.time.com/2011/11/15/the-man-who-invented-email/ Retrieved October 29, 2013.
- Saigal R. Lokvani talks to Dr. Shiva Ayyadurai. Available at http://www.lokvani.com/lokvani/article.php?article_id=4379 Retrieved October 29, 2013.
- Schwimmer J. Why doctors don't email patients. Available at: http://www.healthline.com/health-blogs/tech-medicine/why-doctors-dont-email-patients Retrieved on October 29, 2013.
- Sittig DF. Results of a content analysis of electronic messages (email) sent between patients and their physicians. BMC Med Inform Decis Mak. 2003;3:11.
doi pubmed - White CB, Moyer CA, Stern DT, Katz SJ. A content analysis of e-mail communication between patients and their providers: patients get the message. J Am Med Inform Assoc. 2004;11(4):260-267.
doi pubmed - Anand SG, Feldman MJ, Geller DS, Bisbee A, Bauchner H. A content analysis of e-mail communication between primary care providers and parents. Pediatrics. 2005;115(5):1283-1288.
doi pubmed - ACOG Committee Opinion. Number 365 May 2007. Seeking and giving consultation. Obstet Gynecol. 2007;109(5):1255-1260.
pubmed - ACOG Committee Opinion No. 492: Effective patient-physician communication. Obstet Gynecol. 2011;117(5):1254-1257.
doi - U.S. Department of Health and Human Services. Affordable Care Act 2010. Available at https://www.healthcare.gov Retrieved on October 29, 2013.
- Kane B, Sands DZ. Guidelines for the clinical use of electronic mail with patients. The AMIA Internet Working Group, Task Force on Guidelines for the Use of Clinic-Patient Electronic Mail. J Am Med Inform Assoc. 1998;5(1):104-111.
doi pubmed - Baron RJ. What's keeping us so busy in primary care? A snapshot from one practice. N Engl J Med. 2010;362(17):1632-1636.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.