







| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Case Report
Volume 5, Number 1, March 2016, pages 37-40
Transient Osteoporosis of the Knees, Ankles and Feet: Atypical Case in a Twin Pregnancy
Tatiana Elizabeth Carranco-Medinaa, b, c, Ismael Calero-Paniaguaa, b, Cristina Hidalgo-Callejaa, b, Maria Dolores Sanchez-Gonzaleza, b, Carlos Alberto Montilla-Moralesa, b, Alba Quesada-Morenoa, b, Ricardo Usategui-Martinb, Laura Perez-Garridoa, b, Susana Gomez-Castroa, b, Olga Martinez-Gonzaleza, b, Javier Del Pino-Montesa, b
aHospital Universitario de Salamanca, Rheumatology Department, Spain
bSalamanca Institute for Biomedical Research, IBSAL, Spain
cCorresponding Author: Tatiana Elizabeth Carranco-Medina, Hospital Universitario de Salamanca, Rheumatology Department, Spain
Manuscript accepted for publication October 02, 2015
Short title: Transient Osteoporosis of the Knees
doi: http://dx.doi.org/10.14740/jcgo357w
| Abstract | ▴Top |
Transient osteoporosis (TO) is a rare entity with unknown origin which is, in most cases, self-limiting. The most common location is the hip, which can sometimes be bilateral, followed by the knee, ankle and foot. The multifocal, bilateral and simultaneous location of knees, ankles and feet during pregnancy is extremely rare. We present the case of a woman, 25 weeks pregnant with twins, who was admitted as an emergency with pain and functional disability of her lower limbs. She required hospitalization and was diagnosed with transient osteoporosis of pregnancy (TOP), with clinical and radiological resolution after 12 months and treatment with intravenous bisphosphonate.
Keywords: Transient osteoporosis; Transient bone marrow edema syndrome; Pregnancy; Twins
| Introduction | ▴Top |
Transient osteoporosis (TO) is a rare disease which may affect middle-aged men and pregnant women in their third trimester or after delivery [1, 2]. Some of the terms commonly used to describe this medical entity are transient bone marrow edema syndrome, transitory bone demineralization, regional migratory osteoporosis, reflex sympathetic dystrophy, etc. [3]. It presents with spontaneous joint pain and functional loss without a previous traumatic record. Simple X-rays and bone scintigraphy are useful to confirm a diagnosis, and magnetic resonance imaging (MRI) is the most sensitive technique [3, 4].
The incidence and prevalence of this condition is unknown given the lack of published series, and there are only some isolated cases reported in pregnant women. Curtiss and Kincaid published the first cases in 1959 [5] and, since them, several cases have been reported with the hip joint as the most common location, followed by the knee, ankle and foot. There are few published articles with a simultaneous involvement of both joints of the lower limbs. Our case presents a woman pregnant with twins with simultaneous bilateral involvement of knees, ankles and feet.
| Case Report | ▴Top |
The patient is a 36-year-old woman, 25 weeks pregnant with twins, who was admitted as an emergency with intense pain on the knees and ankles, without a previous record of trauma, associated with functional disability for standing and walking, which required hospitalization. The physical examination revealed intense pain on palpation and on mobilization of knees and ankles. No joint effusion was observed and the meniscal maneuvers were negative. Muscle strength and sensitivity were normal. The knee ultrasound was also normal, and the MRI of the right knee showed a slight joint effusion with bone edema on the subchondral region of the patella and the internal femoral condyle, with a small image of a microfracture (Fig. 1). The analysis revealed hypercalcemia of 11.3 g/dL, vitamin D of 15 mg/dL, and hypercalciuria of 665 mg/day. Complementary tests were performed and a malignant process was ruled out.
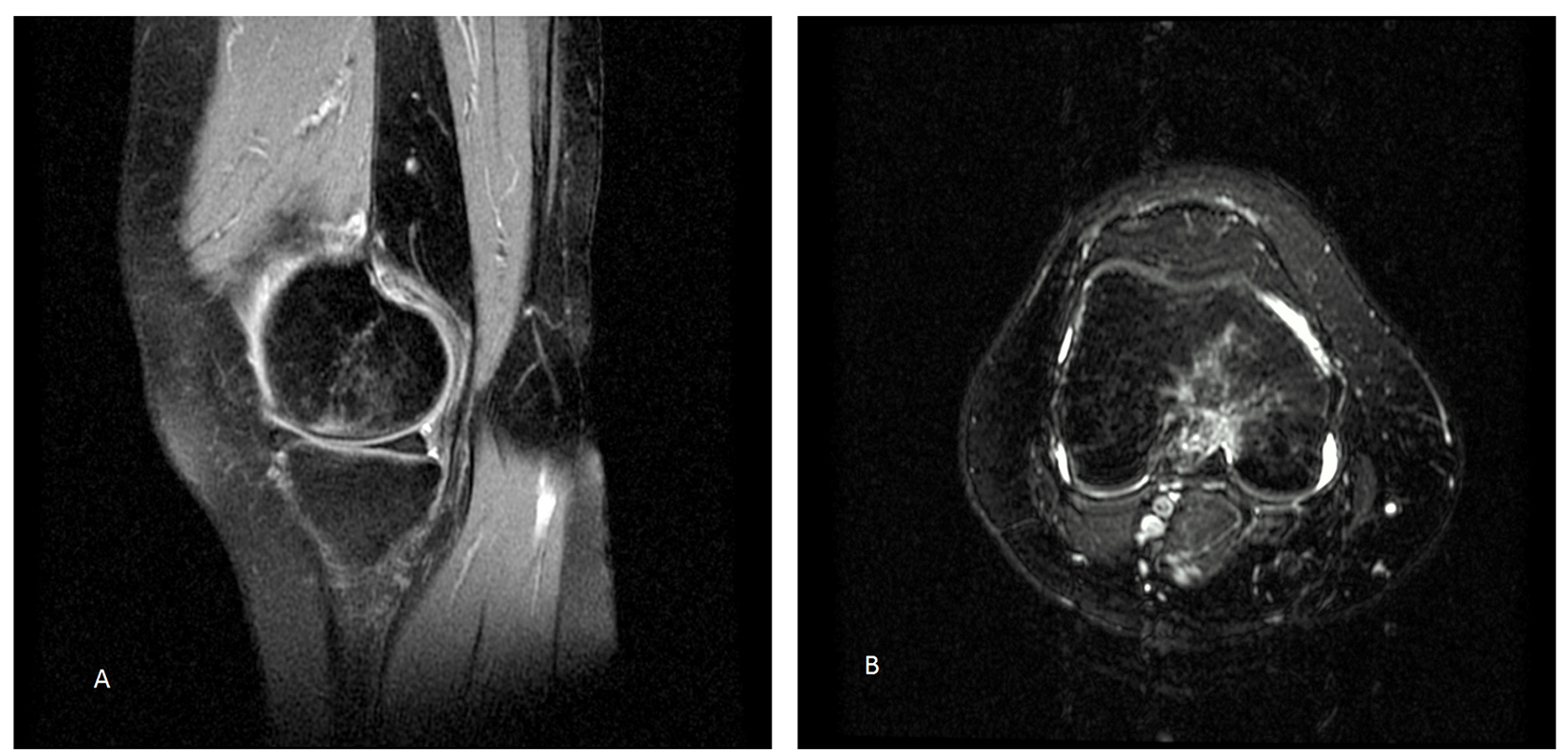 Click for large image | Figure 1. MRI in T2. Enhanced signal on the internal femoral condyle: (A) sagittal section and (B) axial section. |
After a diagnosis of osteoporosis of pregnancy (TOP), treatment was started with analgesics, topical capsaicin and rest. The patient did not report a clinical improvement and she presented with class IV functional capacity. A programmed cesarean section was performed in week 35 of pregnancy. In the postoperative period, X-rays of knees, ankles and feet were obtained (Fig. 2), as well as a bone scintigraphy (Fig. 3). Given the findings and the clinical symptoms, which were resistant to the usual treatment, a 5 mg dose of intravenous zoledronic acid was administered, associated with calcium, vitamin D and rehabilitation.
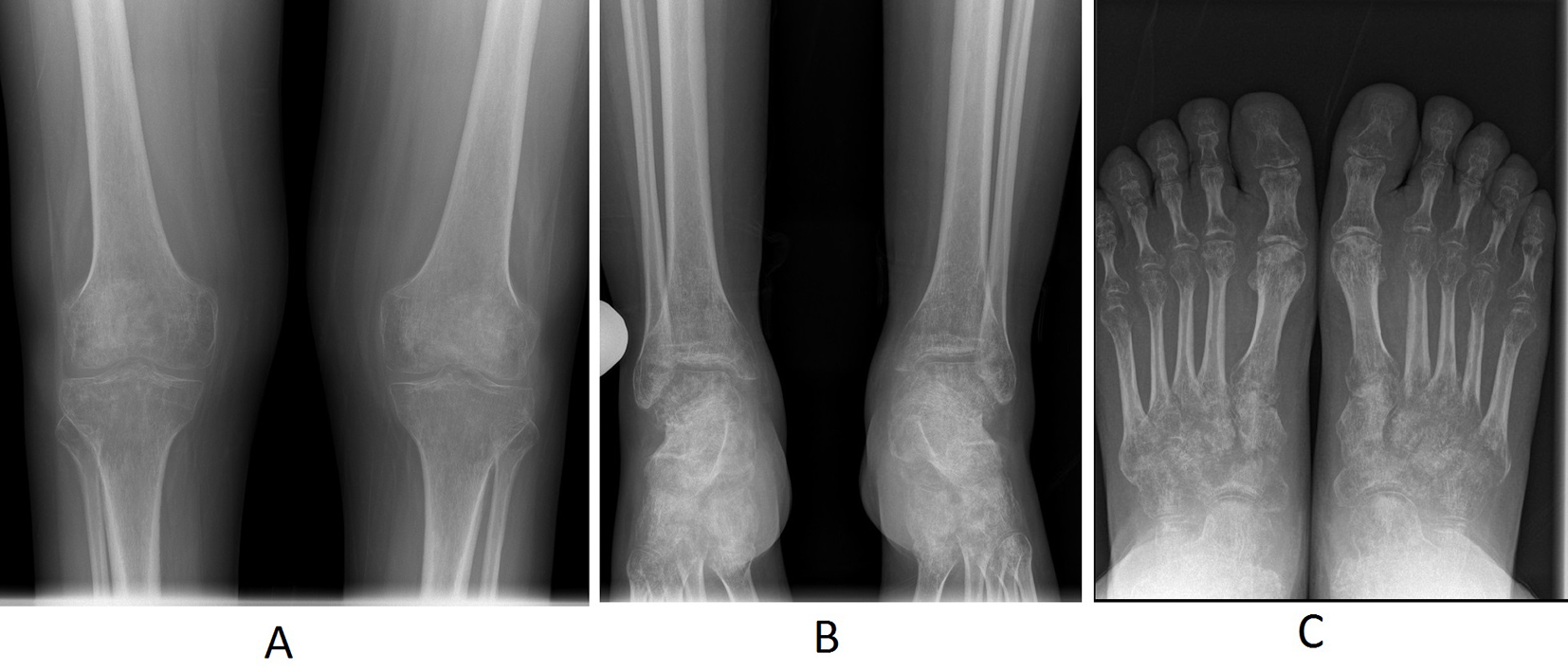 Click for large image | Figure 2. AP simple X-ray: (A) diffuse osteopenia on the distal femoral metaphysis and epiphysis and on the proximal tibia and fibula; (B) patchy osteopenia on the distal metaphysis and epiphysis of tibia and fibula and on tarsi; (C) patchy osteopenia on tarsal bones, head and base of metatarsal bones and phalanges. |
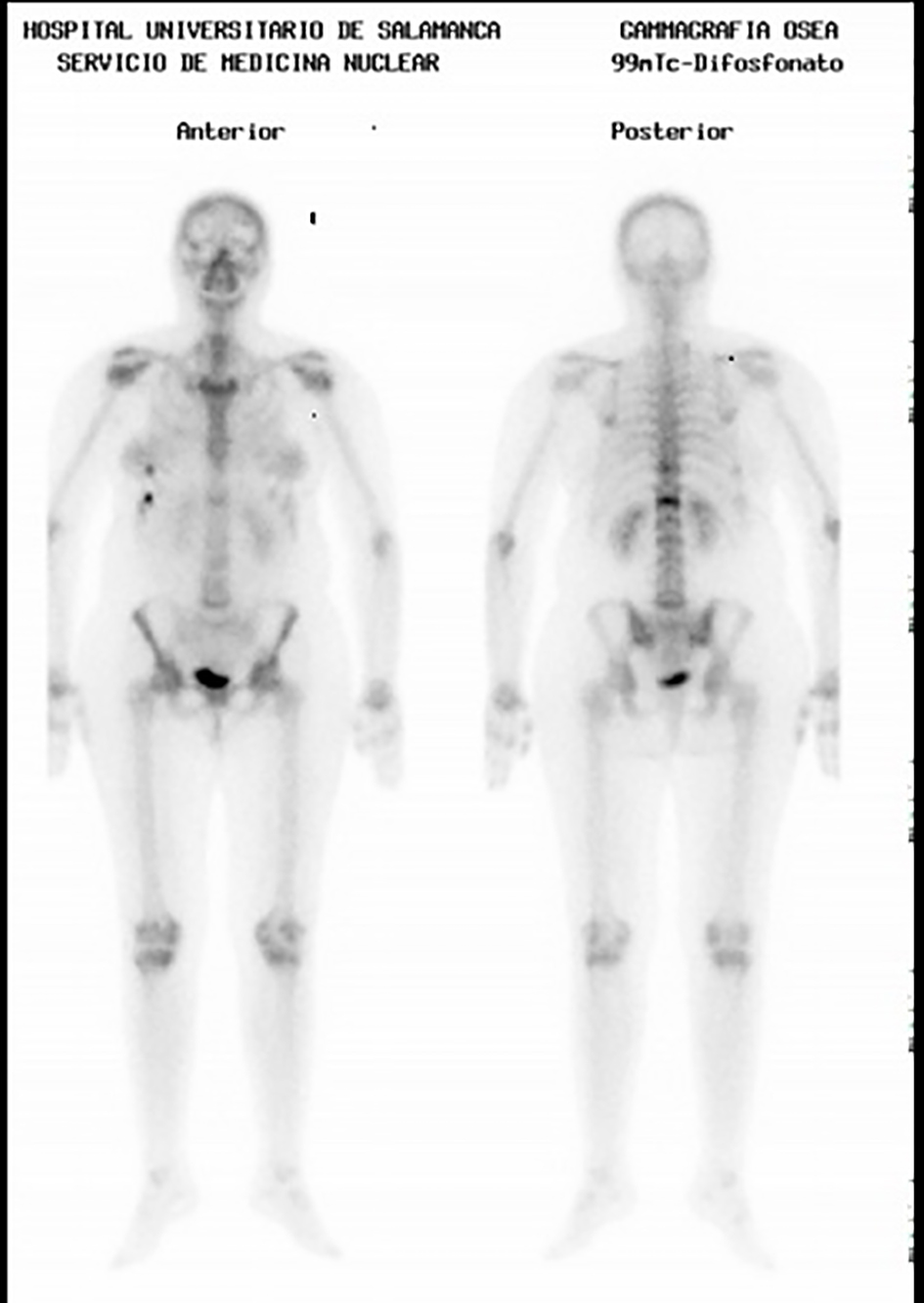 Click for large image | Figure 3. Bone scintigraphy with technetium 99: enhancement of the tracer on the knees, ankles, tarsal and metatarsal bones. |
The control bone scintigraphy which was performed 3 months later detected a lower enhancement of technetium 99 tracer (Fig. 4), as well as normal figures for Ca and vitamin D in the analytical tests.
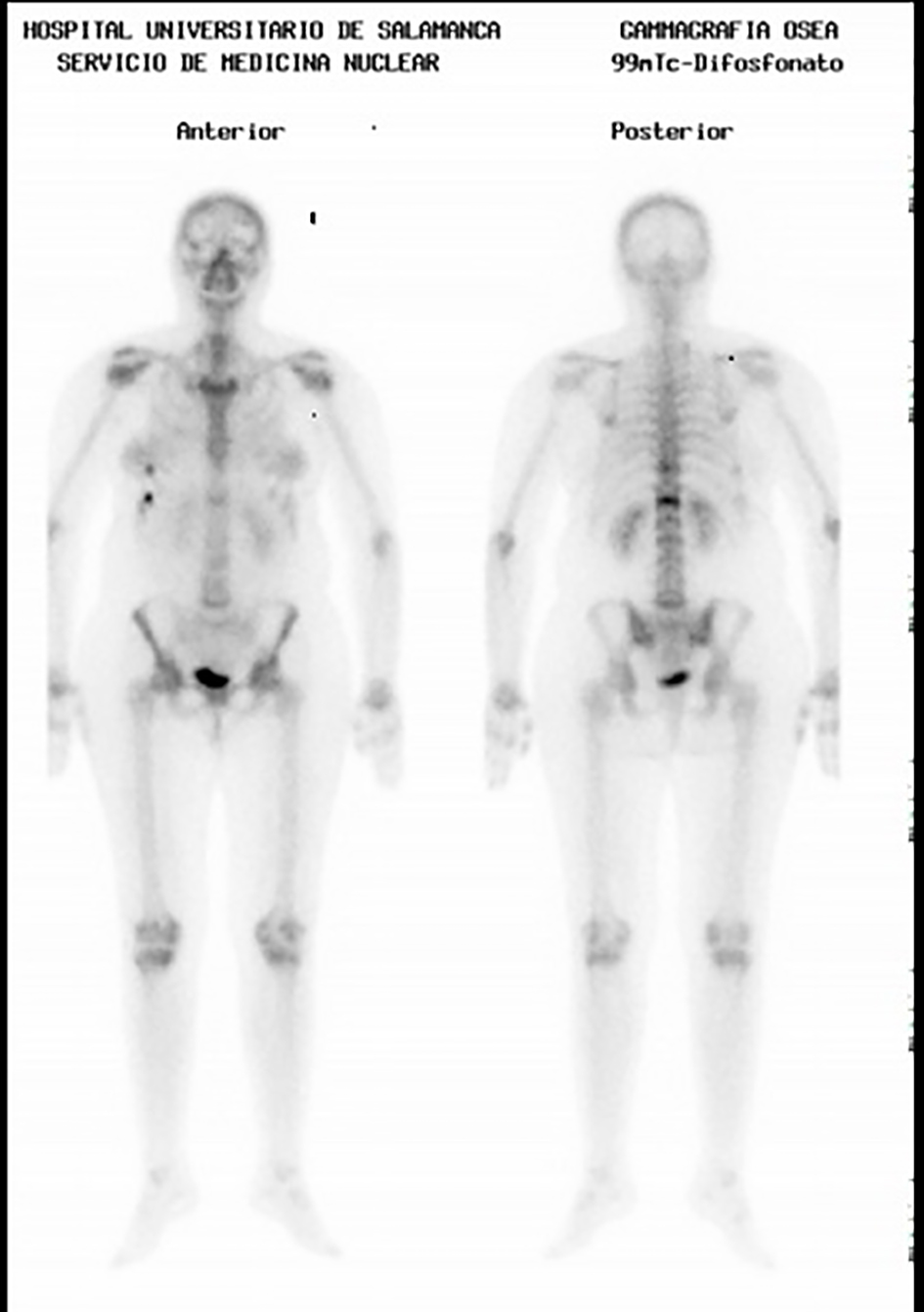 Click for large image | Figure 4. Bone scintigraphy with technetium 99: decreased enhancement of the tracer. |
After 8 months, the patient showed a clinical and radiological improvement (Fig. 5), with functional class I.
 Click for large image | Figure 5. AP simple X-ray: (A) disappearance of patchy osteopenia of the knees; (B) marked reduction of diffuse osteopenia on tarsal and metatarsal bones and on phalanges. |
| Discussion | ▴Top |
TO is a rare entity, but it is cited with increased frequency, and it is probably underdiagnosed. Up to date, there are no adequate epidemiological studies, and its incidence is estimated based on the few clinical cases and series which have been published. It is located on the load-bearing joints of the lower limbs: hip (70%), knee, ankle and foot [6]. An involvement of different areas of the same joint is also possible, as well as migration from one joint to another, which is described as regional migratory osteoporosis. From 10 to 40% of patients develop this condition in several joints, either simultaneously or successively, on the same limb or on the contralateral limb. In its most common presentation, it spreads from the proximal to the distal end in the same limb [6-9]. A bilateral simultaneous involvement in both hips is exclusive of pregnant women [9, 10]. Its pathogenesis is unclear and it is suggestive of a multifactorial origin: microtraumatisms, trabecular microfractures caused by a reduction of bone mass during pregnancy, neurovascular dysfunction, joint overload caused by weight gain and hormonal changes typical of pregnancy, resulting in ischemic tissue and bone edema, which are characteristic of this entity [6, 10].
Clinically, it presents with spontaneous pain without a previous traumatic or infectious record, with variable intensity, sudden or insidious onset, which is exacerbated by loads, improves with rest and may deteriorate quickly and progressively until it causes severe functional disability which requires hospitalization. One of its main clinical characteristics is that symptoms and disability are not correlated with clinical findings, although it is sometimes accompanied by inflammation, with soft tissue edema and a slight joint effusion. Fatigue fractures are a rare complication [8].
The analytical study does not generally reveal alterations, except for those typical of pregnancy. In our case, hypercalcemia might be due to the large extension of the bone involvement and the immobility caused by the severity of the functional disability.
In its first stages, X-rays are not able to detect alterations in bone mineralization although more advanced stages may reveal diffuse osteopenia with preservation of joint spaces. At an early stage, scintigraphy is a more sensitive technique and it shows marked and diffuse hyper-enhancement of the isotope. MRI is an essential tool in diagnosis; it shows bone edema in the affected area, it makes it possible to obtain a differential diagnosis with other processes, mainly infectious and cancerous, and it is also extremely useful during the monitoring stage [6, 7, 10, 11].
Most series highlight the self-limiting nature of symptoms over 6 - 12 months. However, in some patients, this period may be longer, depending on the extension and severity of the form of presentation as well as on the treatment [6, 11].
The treatment of choice is conservative, with rest, analgesics, anti-inflammatory drugs, unloading and physical therapy. Several drugs have been used in these cases. However, evidence is based on the experience of published clinical cases and case series. Some of the drugs which have been used are bisphosphonates, glucocorticoids, prostaglandins, and calcium antagonists. In the group of bisphosphonates, the most recommended drugs are alendronic acid, pamidronic acid, ibandronic acid and zoledronic acid [10, 12].
Lopez Sagasta et al described the case of a 46-year-old woman pregnant with twins in her third trimester who developed a unilateral transient bone edema of the knee with spontaneous resolution after 8 - 9 months [13]. Our case is atypical due to the simultaneous and bilateral involvement of several joints of the lower limbs. We also believe that the twin pregnancy contributed to this aggressive form of presentation and that the adequate postpartum treatment with intravenous bisphosphonates improved the evolution of this condition.
It is necessary to rule out the presence of TO in all pregnant women who, in their third trimester, present with permanent pain of one joint which is mechanical, progressively disabling and disproportionate to the clinical signs.
An early diagnosis with the use of scintigraphy and MRI, whenever the circumstances allow it, is important. Also, an early treatment is essential for a quick recovery from the process and to prevent complications such as fractures.
| References | ▴Top |
- Ververidis AN, Drosos GI, Kazakos KJ, Xarchas KC, Verettas DA. Bilateral transient bone marrow edema or transient osteoporosis of the knee in pregnancy. Knee Surg Sports Traumatol Arthrosc. 2009;17(9):1061-1064.
doi pubmed - Charpidou T, Lang F, Langenegger T, Dedes KJ, Honegger C. Bilateral transient osteoporosis of the knee during pregnancy. Arch Gynecol Obstet. 2013;287(6):1259-1261.
doi pubmed - Lakhanpal S, Ginsburg WW, Luthra HS, Hunder GG. Transient regional osteoporosis. A study of 56 cases and review of the literature. Ann Intern Med. 1987;106(3):444-450.
doi pubmed - Lazaro AA, Giraldez MA, Borrego E, Del Rio M, Andres MA, Ribera J. Sindrome de edema de medula osea en mujeres embarazadas: serie de casos y revision de la literatura. Rev S And Traum y Ort. 2012;29:9-15.
- Curtiss PH, Jr., Kincaid WE. Transitory demineralization of the hip in pregnancy. A report of three cases. J Bone Joint Surg Am. 1959;41-A:1327-1333.
pubmed - Patel S. Primary bone marrow oedema syndromes. Rheumatology (Oxford). 2014;53(5):785-792.
doi pubmed - Massara A, Orzincolo C, Prandini N, Trotta F. [Transient regional osteoporosis]. Reumatismo. 2005;57(1):5-15.
pubmed - Aynaci O, Kerimoglu S, Ozturk C, Saracoglu M. Bilateral non-traumatic acetabular and femoral neck fractures due to pregnancy-associated osteoporosis. Arch Orthop Trauma Surg. 2008;128(3):313-316.
doi pubmed - Bruscas Izu C, San Juan de la Parra S. Transient osteoporosis of both hips in pregnancy. Reumatol Clin. 2014;10(1):58-59.
doi pubmed - Reese ME, Fitzgerald C, Hynes C. Transient osteoporosis of pregnancy of the bilateral hips in twin gestation: a case series. PM R. 2015;7(1):88-93.
doi pubmed - Suresh SS. Migrating bone marrow edema syndrome: a cause of recurring knee pain. Acta Orthop Traumatol Turc. 2010;44(4):340-343.
doi pubmed - Seok H, Kim YT, Kim SH, Cha JG. Treatment of transient osteoporosis of the hip with intravenous zoledronate - a case report. Ann Rehabil Med. 2011;35(3):432-435.
doi pubmed - Lopez Sagasta L, Torres Campos A, Seral Garcia B, Albareda Albareda J. Osteoporosis transitoria de rodilla en el embarazo. Rev Esp Cir Osteoart. 2013;255:128-131.
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.