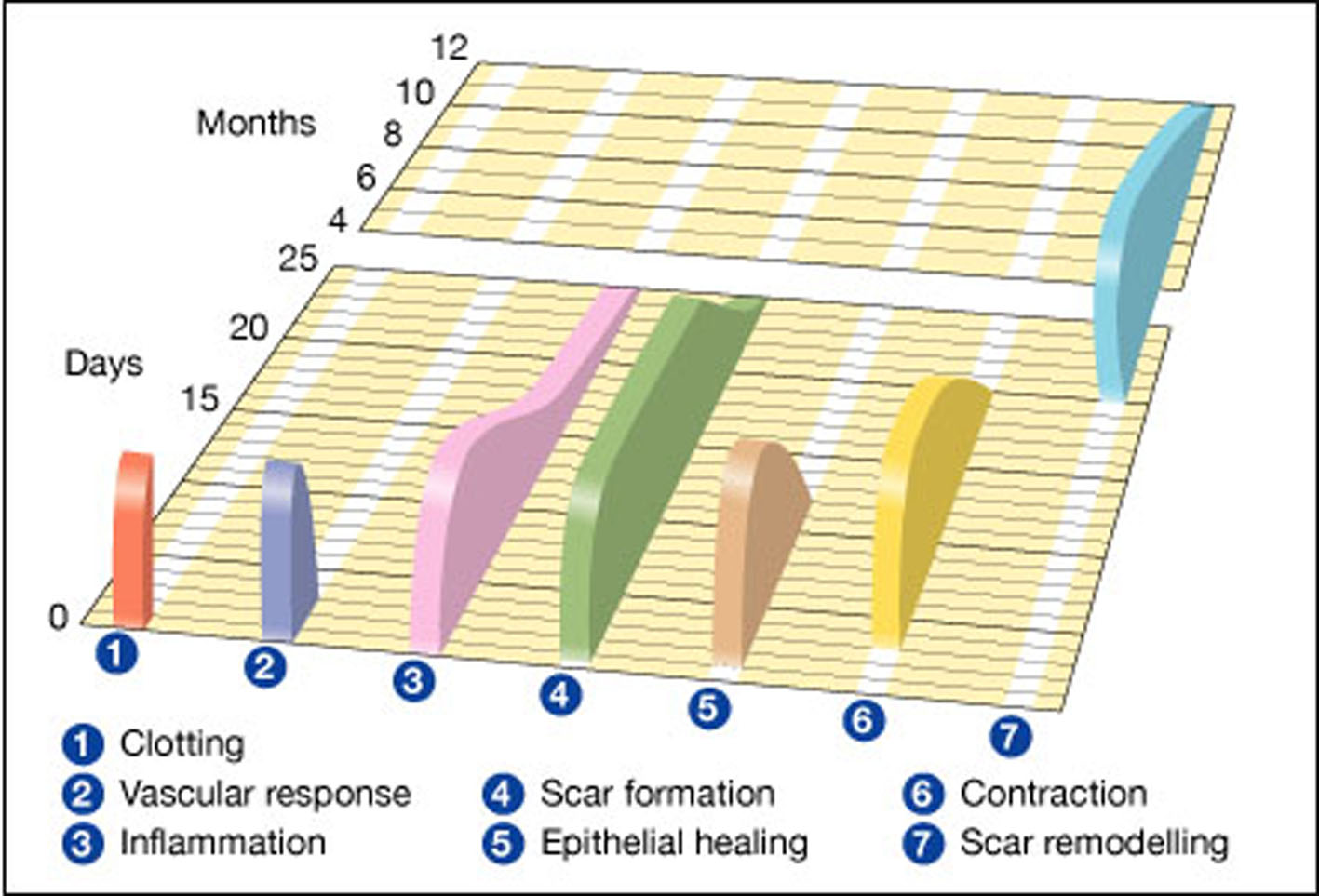
Figure 1. Wound healing phases against a timeline. 1 and 2 represent the hemostatic phase and 4, 5 and 6 represent the proliferation phase. Gregory S. Schultz, Glenn Ladwig and Annette Wysocki - adapted from Asmussen PD, Sollner B [6].
| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Review
Volume 4, Number 2, June 2015, pages 197-202
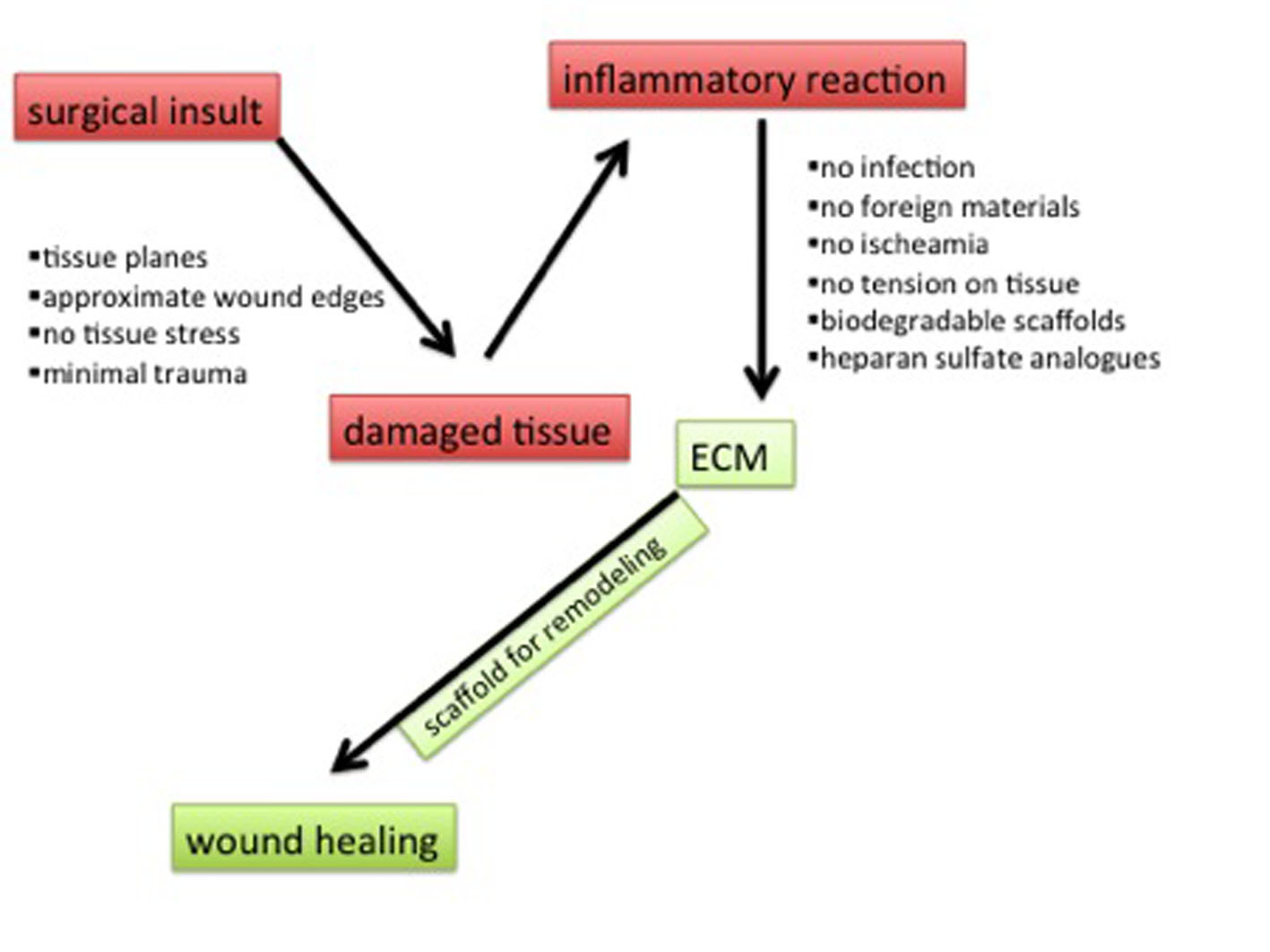
Native Tissue Repair and Principles of Wound Healing: Introducing the Concept of Regenerative Surgery in Vaginal Prolapse Repair
Figures