Figures

Figure 1. Pelvic MRI images of T2 intensified (1-1: sagittal section; 1-2: transverse section). Uterine cervical tumor of 3 cm in diameter was visualized on MRI (arrow). The tumor invaded to the right parametrial space with interruption of the stromal ring (arrow in 2-2). The MRI indicates stage IIB cervical cancer.
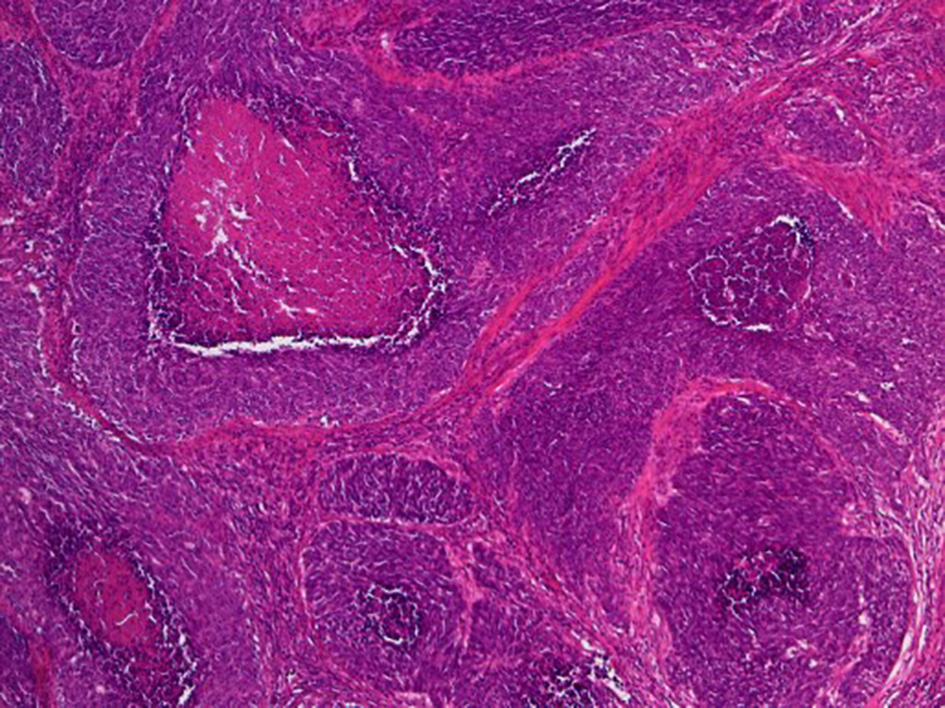
Figure 2. Histological findings of surgical specimen of cervical tumor (H&E stain, original magnification × 40). Relatively large tumor cells invasively proliferate with organoid nesting pattern and central necrosis.
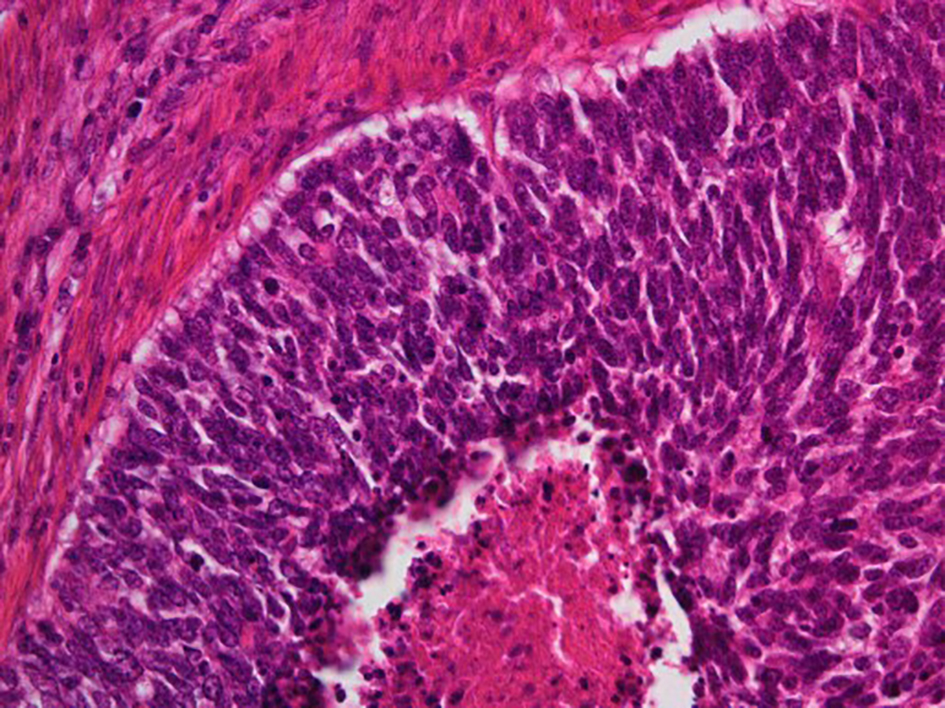
Figure 3. Histological findings of surgical specimen of cervical tumor (H&E stain, original magnification × 200). Peripheral nuclear palisading and central necrosis are histologically observed.
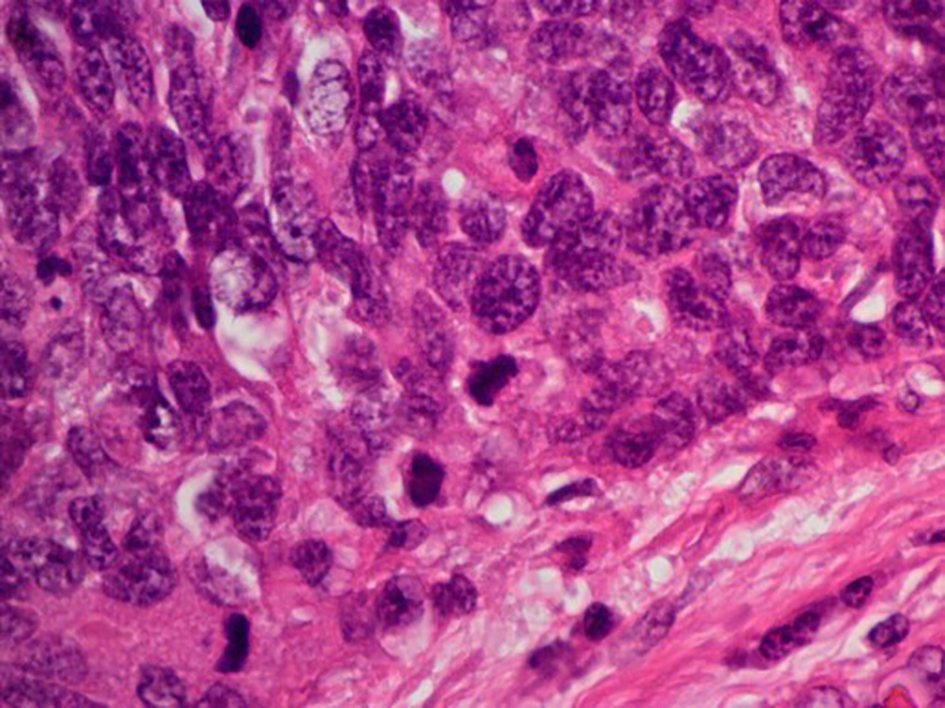
Figure 4. Histological findings of surgical specimen of cervical tumor ( H&E stain, original magnification × 400). Tumor cells exhibit abundant cytoplasm with vesicular nuclei. Mitotic activity of the tumor cell was high.
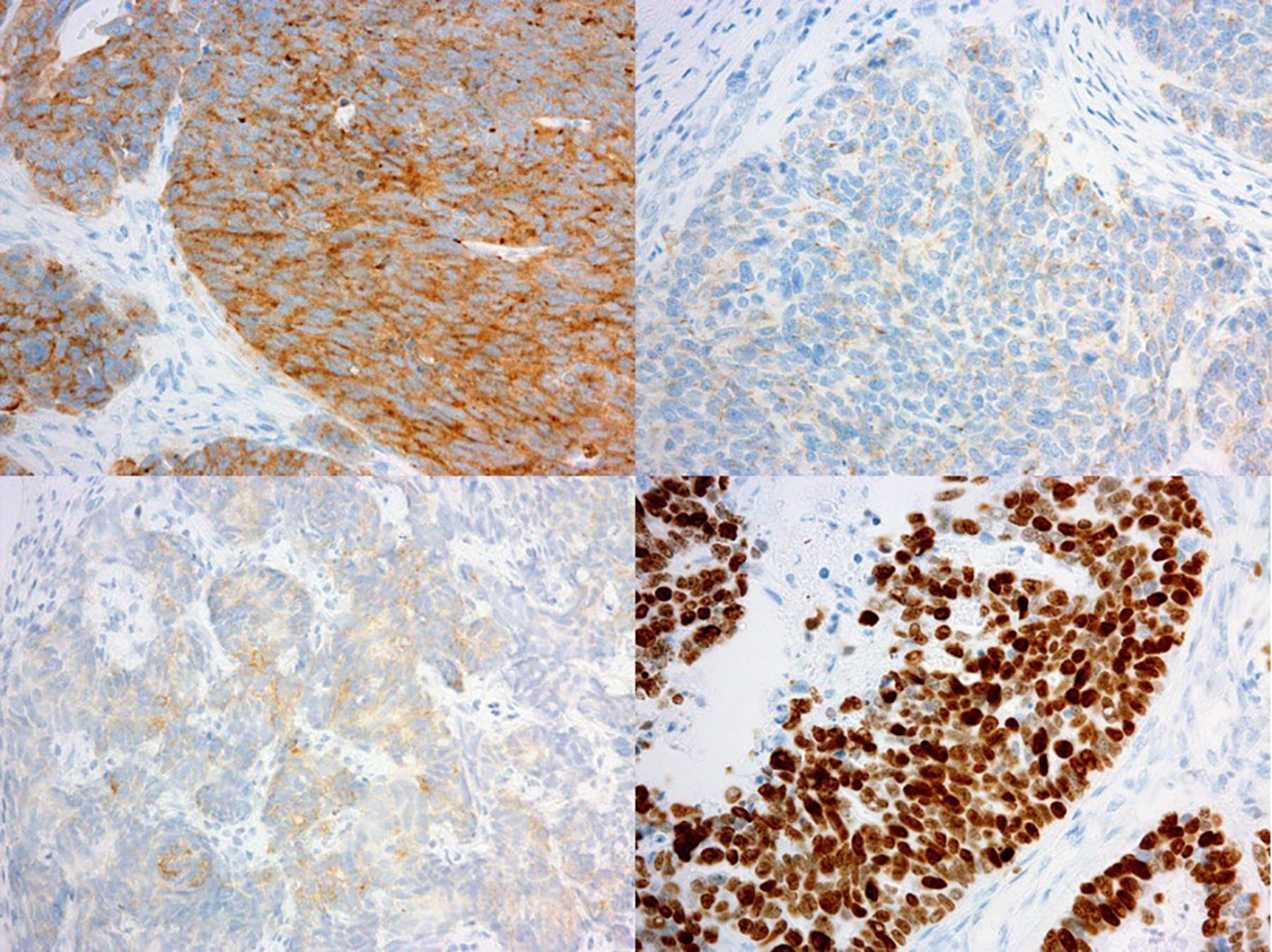
Figure 5. Immunohistochemical findings of surgical specimen of cervical tumor (immunohistochemistry, original magnification × 100). Immunohistochemical staining of the tumor was strongly positive for synaptophysin (upper left), weakly positive for chromogranin-A (upper right) and partially positive for NCAM (bottom left). The Ki-67 index of the tumor cells was almost 100% (bottom right).