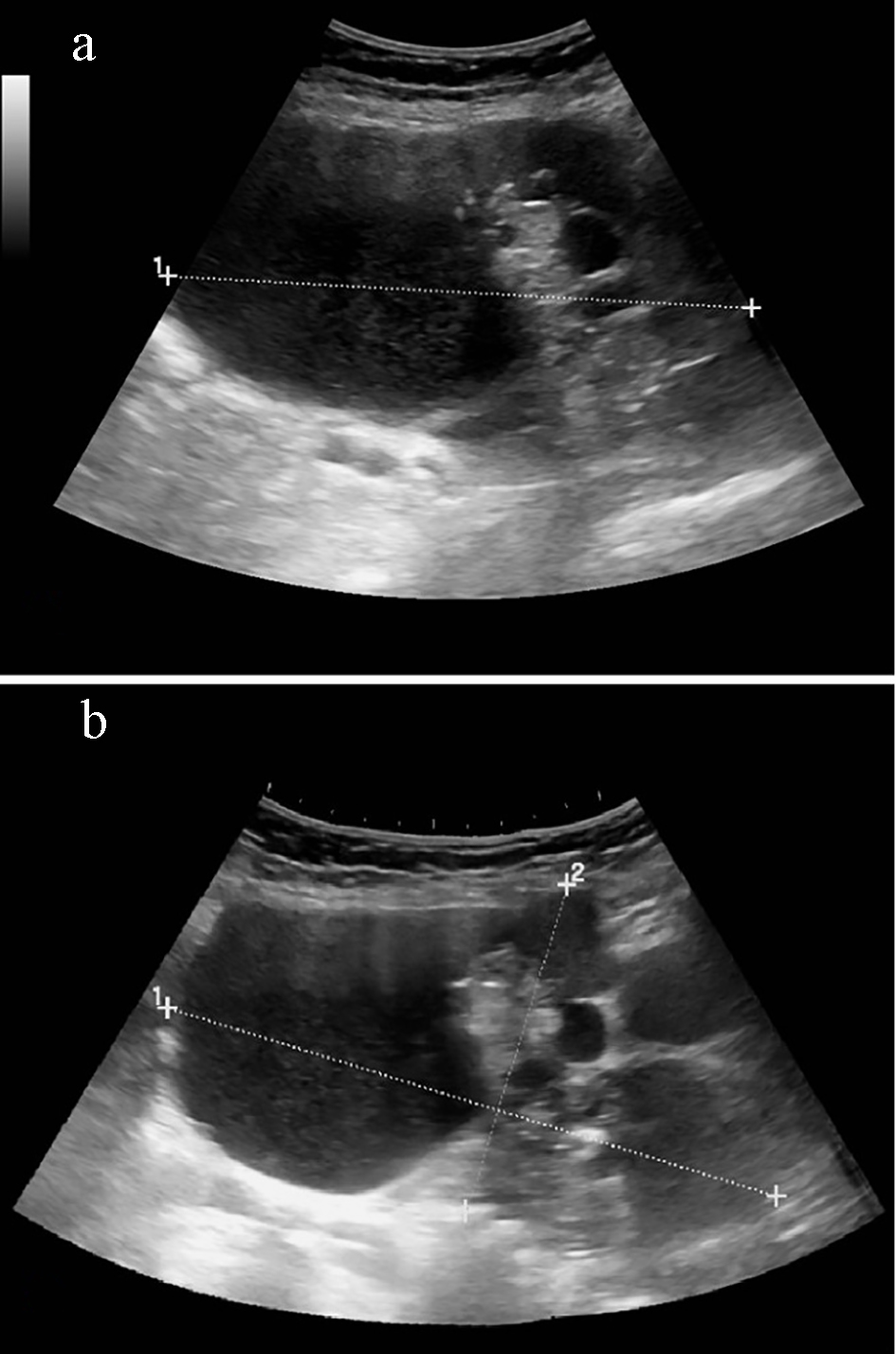
Figure 1. (a) Complex heterogenous pelvic mass with predominantly cystic and some solid echogenic areas measuring 18.68 × 13.72 × 9.76 cm (transverse view). (b) Mass involves both right and left adnexal regions and extends superiorly into the abdominal cavity (sagittal view).