

| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Case Report
Volume 5, Number 1, March 2016, pages 50-52
Notching in the Umbilical Artery Doppler Waveform in the Absence of Cord and Placental Structural Abnormalities: A Case of Massive Fetomaternal Hemorrhage
Mai Nishimuraa, Ayaka Nakashimaa, Kayoko Shikadoa, Kazuhide Ogitaa, b
aDepartment of Obstetrics and Gynecology, Rinku General Medical Center, Osaka, Japan
bCorresponding Author: Kazuhide Ogita, Department of Obstetrics and Gynecology, Rinku General Medical Center, 2-23, Rinku Orai Kita, Izumisano City, Osaka 598-8577, Japan
Manuscript accepted for publication February 04, 2016
Short title: Umbilical Artery Doppler Waveform
doi: http://dx.doi.org/10.14740/jcgo386w
| Abstract | ▴Top |
Massive fetomaternal hemorrhage can cause severe anemia and fetal death. Early diagnosis and blood transfusion can prevent life-threatening events. We describe a case of massive fetomaternal hemorrhage in a previously well primigravida who visited our hospital with a chief complaint of decreased fetal movements and presented with a sinusoidal fetal heart rate pattern in the cardiotocographic tracings. The umbilical artery Doppler waveform showed notching, and the peak systolic velocity of the fetal middle cerebral artery (MCA) was normal. Emergency cesarean section was performed; however, the neonate died despite providing life-support. Thus, we recommend consideration of impending fetal death in patients with non-reassuring fetal heart rate and notching in the umbilical artery Doppler waveform even in the absence of increased peak systolic velocity of the fetal MCA.
Keywords: Doppler; Notching; Umbilical artery; Waveform; Fetomaternal hemorrhage
| Introduction | ▴Top |
Massive fetomaternal hemorrhage can cause severe anemia and fetal death. Early diagnosis and blood transfusion can prevent life-threatening events. We describe a case of massive fetomaternal hemorrhage which resulted in neonatal death. The important point of this case is that non-reassuring fetal heart rate tracings and notching in the umbilical artery Doppler waveform should be considered important even in the absence of increased peak systolic velocity of the fetal middle cerebral artery (MCA) because it might indicate impending fetal death.
| Case Report | ▴Top |
A previously well 19-year-old primigravida at 34 + 4 weeks gestation visited our hospital with a chief complaint of decreased fetal movements for approximately past 12 h. She had no abdominal pain or vaginal bleeding, and had no history of trauma. The patient had received routine prenatal care. She had no remarkable medical and family history. Her cardiotocographic tracings indicated a sinusoidal fetal heart rate pattern. Ultrasound examination with an LOGIQ P6 machine (GE Healthcare, Milwaukee, WI) and a 5-MHz curvilinear transducer showed a fetus with cephalic presentation and growth appropriate for its gestational age. Biophysical profile examination of the fetus revealed a score of 2/8. The only normal component was the amniotic fluid index of 12.07. There were no anatomical abnormalities and no signs of hydrops fetalis. Doppler measurement of the peak systolic velocity of the fetal MCA blood flow was 40.5 cm/s. The fetal MCA pulsatility index (PI) and the resistance index (RI) were 1.13 and 0.64, respectively, suggestive of slightly decreased vascular resistance. The umbilical artery Doppler waveform showed notching (Fig. 1). The umbilical artery PI and RI were 0.77 and 0.53, respectively. Laboratory test results revealed normal complete blood count, blood chemistry, and coagulation profile. Fetal hemoglobin concentration was 7.3%, suggestive of massive fetomaternal hemorrhage. Estimated blood volume projected from fetal circulation to maternal circulation was more than 250 mL. Her blood type was A Rh+. Coombs test results were negative.
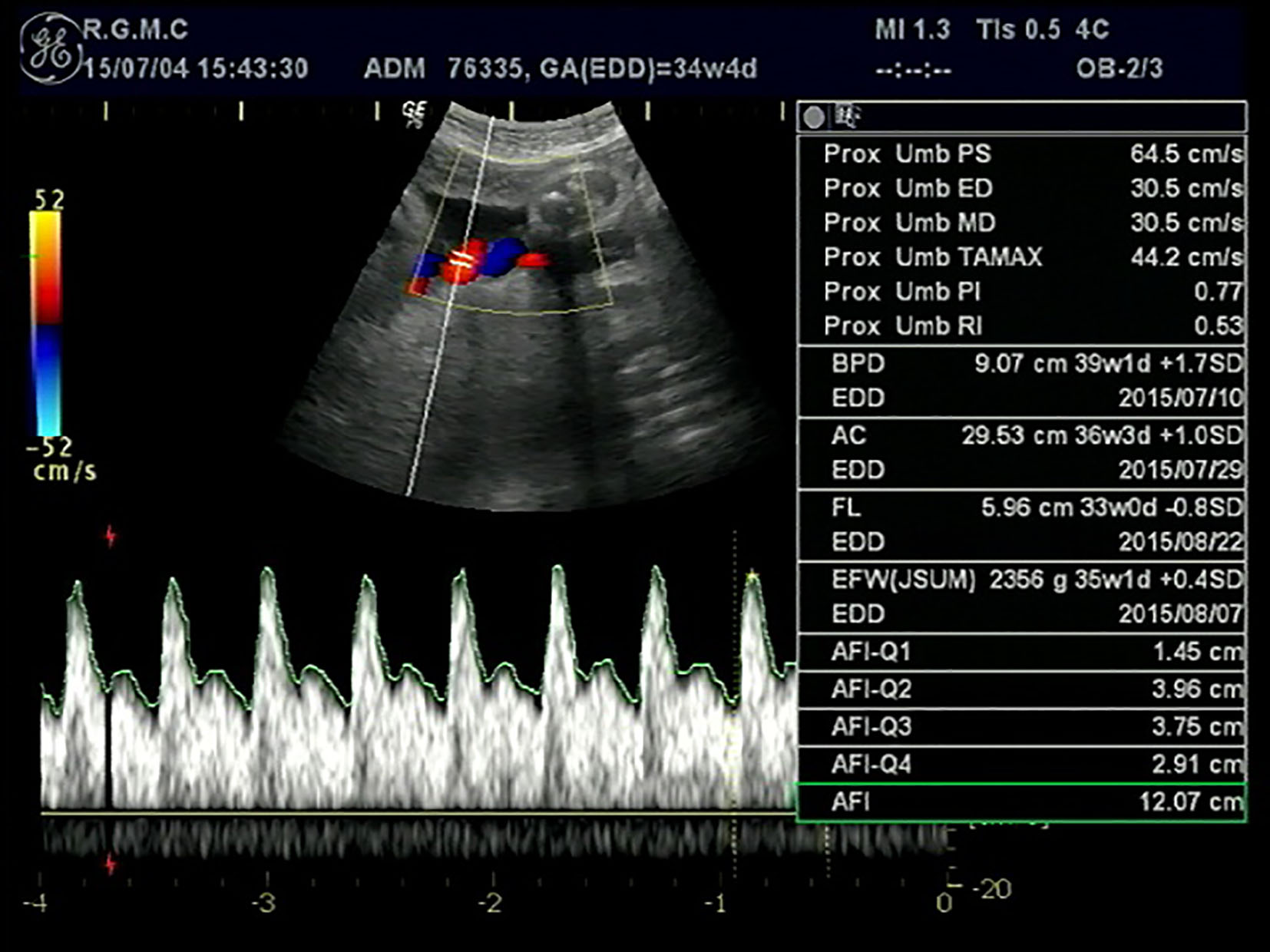 Click for large image | Figure 1. The umbilical artery Doppler waveform showing notching. |
Emergency cesarean section was performed under spinal anesthesia. A male infant weighing 2,640 g was delivered; its 1- and 5-min Apgar scores were 1 and 2, respectively. Entanglement of the cord around the fetal parts was not detected. There was no macroscopic evidence of placental abruption, knot formation, entanglement, and marginal or velamentous insertion. The hemoglobin concentration of the neonate was 2.9 g/dL and his blood type was A Rh+. The neonatologists performed intubation and volume resuscitation; however, the neonate died about 1.5 h later.
The placenta appeared anemic on gross examination and multiple hematomas in the intervillous spaces were found on pathological examination. The final diagnosis was massive fetomaternal hemorrhage.
| Discussion | ▴Top |
Umbilical artery waveform notching has been reported previously in association with cord entanglement in velamentous cord insertion [1], knot formation [2], monoamniotic twins [3, 4], and umbilical artery compression [5]. Abuhamad and co-authors reported that umbilical artery waveform notching suggests cord and placental abnormalities, and more importantly, is associated with non-reassuring fetal heart rate tracings and emergency cesarean sections [6].
The plausible cause for notching in the umbilical artery Doppler waveform is constriction. Tejada-Martinez and co-authors used computational fluid dynamic analysis and concluded that waveform notching is caused by flow separation induced by constriction [7, 8]. The notching is not present in cases of less than 75% constriction and disappears as the vortex wave is attenuated at distances downstream of the constriction. In flows with 75% and 85% constriction, the notching disappears at distances shorter than 3.8 and 4.3 cm downstream of the constriction, respectively.
Massive fetomaternal hemorrhage is rare, but results in serious complications including severe fetal anemia, hydrops fetalis, and even fetal death. As described in the literature, ultrasound findings of fetal anemia include increased peak flow velocity of the fetal MCA and coronary arteries and reversed end-diastolic flow in the fetal MCA [9, 10]. To our knowledge, this is the first report of umbilical artery waveform notching in women with massive fetomaternal hemorrhage. The actual mechanism for the notching in massive fetomaternal hemorrhage was not clear; however, we would speculate that umbilical artery spasm in compensation to acute and severe fetal anemia caused the notching in the umbilical artery waveform. In this case, peak systolic velocity of the fetal MCA, MCA-PI, and MCA-RI were within normal limits. We assumed that this was because the fetal hemorrhage was so massive and acute that the fetal compensation was not able to work.
This case suggests that non-reassuring fetal heart rate tracings and notching in the umbilical artery Doppler waveform should be considered important even in the absence of increased peak systolic velocity of the fetal MCA because it might indicate impending fetal death.
Conflicts of Interest
Authors declare no conflicts of interest associated with this article.
| References | ▴Top |
- Robinson JN, Abuhamad AZ, Sayed A, Evans AT. Umbilical artery Doppler velocimetry waveform notching and umbilical cord abnormalities. J Ultrasound Med. 1997;16(5):373-375.
doi pubmed - Jakobi P, Weiner Z, Goren T, Thaler I. Systolic notch in umbilical artery flow velocity waveforms associated with a tight true knot of the cord. J Matern Fetal Investig. 1994;4:119-121.
- Abuhamad AZ, Mari G, Copel JA, Cantwell CJ, Evans AT. Umbilical artery flow velocity waveforms in monoamniotic twins with cord entanglement. Obstet Gynecol. 1995;86(4 Pt 2):674-677.
doi - Kofinas AD, Penry M, Hatjis CG. Umbilical vessel flow velocity waveforms in cord entanglement in a monoamnionic multiple gestation. A case report. J Reprod Med. 1991;36(4):314-316.
pubmed - Robinson JN, Abuhamad AZ, Evans AT. Umbilical artery Doppler velocimetry waveform abnormality in fetal gastroschisis. Ultrasound Obstet Gynecol. 1997;10(5):356-358.
doi pubmed - Abuhamad A, Sclater AJ, Carlson EJ, Moriarity RP, Aguiar MA. Umbilical artery Doppler waveform notching: is it a marker for cord and placental abnormalities? J Ultrasound Med. 2002;21(8):857-860.
pubmed - Adamson SL, Morrow RJ, Bascom PA, Mo LY, Ritchie JW. Effect of placental resistance, arterial diameter, and blood pressure on the uterine arterial velocity waveform: a computer modeling approach. Ultrasound Med Biol. 1989;15(5):437-442.
doi - Tejada-Martinez AE, Borberg CJ, Venugopal R, Carballo C, Moreno WA, Quintero RA. Computational fluid dynamic analysis of flow velocity waveform notching in umbilical arteries. Am J Physiol Regul Integr Comp Physiol. 2011;300(1):R76-84.
doi pubmed - Baschat AA, Harman CR, Alger LS, Weiner CP. Fetal coronary and cerebral blood flow in acute fetomaternal hemorrhage. Ultrasound Obstet Gynecol. 1998;12(2):128-131.
doi pubmed - Sueters M, Arabin B, Oepkes D. Doppler sonography for predicting fetal anemia caused by massive fetomaternal hemorrhage. Ultrasound Obstet Gynecol. 2003;22(2):186-189.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.