| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Case Report
Volume 4, Number 3, September 2015, pages 275-278
Highly Elevated Level of Serum CA125 Produced by a Large Uterine Leiomyoma in a 20-Year-Old Woman
Ai Miyoshia, b, Takashi Miyatakea, Shinnosuke Komiyaa, Mayuko Mimuraa, Masaaki Nagamatsua, Takeshi Yokoia
aDepartment of Obstetrics and Gynecology, Kaizuka City Hospital, Oska-fu, Japan
bCorresponding Author: Ai Miyoshi, Department of Obstetrics and Gynecology, Kaizuka City Hospital, 3-10-20 Hori Kaiduka-shi, Oska-fu, 597-0015, Japan
Manuscript accepted for publication June 19, 2015
Short title: Leiomyoma With Elevated CA125
doi: http://dx.doi.org/10.14740/jcgo344w
| Abstract | ▴Top |
A 20-year-old woman presented with a pelvic tumor that caused abdominal protuberance. Transvaginal ultrasonography revealed a 15 cm mass developed from her uterus. Her cancer antigen 125 (CA125) serum level at presentation was 1,570.9 U/mL and lactate dehydrogenase (LDH) level was 377 U/L. The suspicion was of a malignant neoplasm, so we undertook a myomectomy. The pathologic diagnosis was a leiomyoma of the uterus. Both the CA125 and LDH serum levels dropped unusually rapidly to normal after the operation. Immunohistochemical staining for CA125 indicated that the leiomyoma was the source of the high level of serum CA125.
Keywords: CA125; Uterine leiomyoma; Menstrual
| Introduction | ▴Top |
Uterine leiomyoma is a common gynecological disorder, and it is said that 40-60% of women of reproductive age will at some point have one [1]. Although high levels of tumor markers are often found in benign gynecological disease, it does not appear that leiomyomas have previously been associated with specific tumor markers. However, there have been reports of a relationship with serum lactate dehydrogenase (LDH) level. We now report a case of a leiomyoma with a highly elevated level of cancer antigen 125 (CA125) prior to surgery.
| Case Report | ▴Top |
A 20-year-old woman suffering abdominal protuberance consulted her gynecologist. Transvaginal ultrasonography revealed a pelvic tumor. At the first consultation, her serum CA125 level was 1,570.9 U/mL and LDH was 377 U/L. The levels of carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19-9 were within normal range. C-reactive protein (CRP) was modestly increased; however, no other abnormal clinical laboratory results were found. The pelvic tumor was suspected to be malignant and she came to our hospital for medical treatment.
Our transvaginal ultrasonography showed a 15 cm mass developed from the uterus; there was no necrosis present in the tumor and no ascites (Fig. 1). The ovaries were not detected. The MRI results were the same. The diagnosis based solely on imaging analysis was leiomyoma. The high levels of serum CA125 and LDH also gave credence to our suspicion that her tumor was a leiomyosarcoma or adenomatoid tumor.
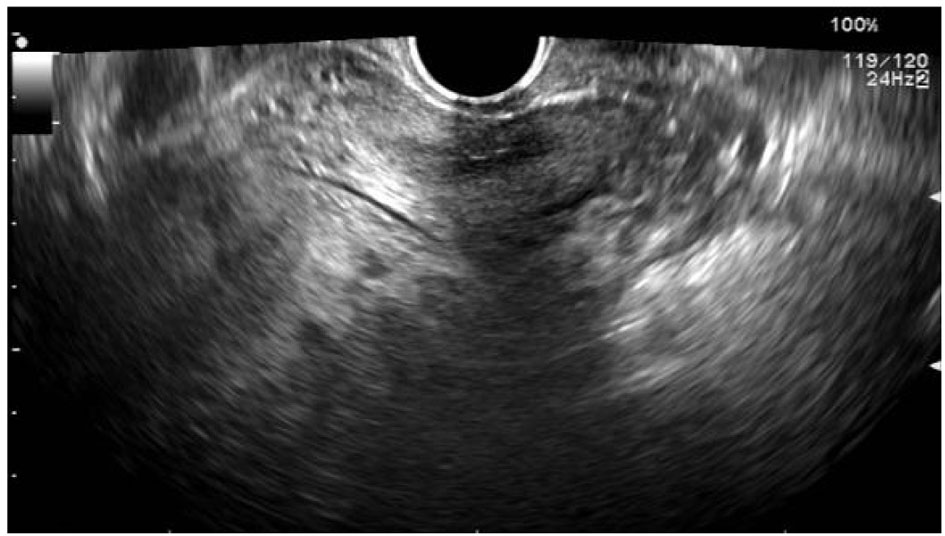 Click for large image | Figure 1. Transvaginal ultrasonography of the pelvic region. A 15 cm mass developed from the uterus is shown. There is no evidence of ascites or necrosis. Neither ovary is detected |
We undertook a myomectomy to obtain a histological diagnosis. At the operation, neither endometriosis nor adenomyosis was detected. The new-born head-sized leiomyoma developing from the upper uterine segment was resected. The pathologic diagnosis was of a non-malignant leiomyoma of the uterus. The hematoxylin-eosin (H&E) staining appearance of the tumor was of a typical leiomyoma. Immunohistological staining showed positivity for CA125, but there was not the luminal structure normally found in an adenomatoid tumor (Fig. 2).
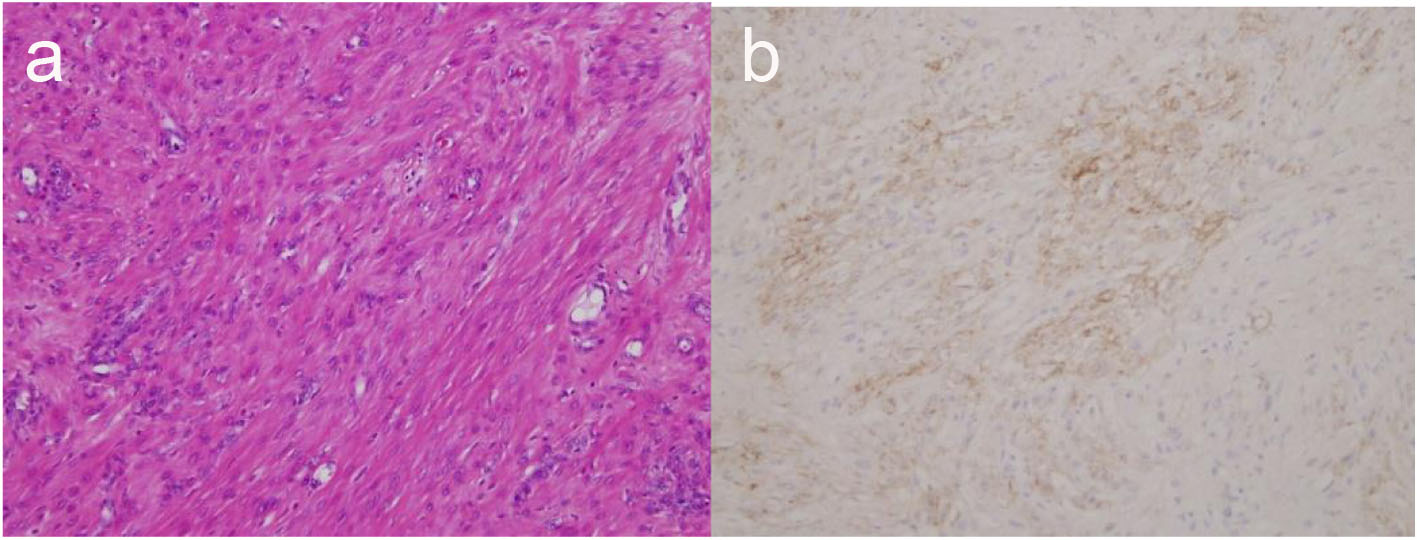 Click for large image | Figure 2. H&E staining (a) and CA125 immunochemistry (b) of the tumor. The spindle-shaped tumor cells have cytologically bland, relatively uniform nuclei with fine chromatin and small nucleoli. The cytoplasm is abundant, eosinophilic and fibrillar (a). CA125 immunostaining of the same slide showed positive staining of the cytoplasm of tumor cells (b). |
After the myomectomy, her elevated serum CA125 level began falling, and dropped to a normal level within 1 month. Her CA125 level has not re-elevated after the operation, even during her menstrual period. Her serum LDH level also returned to a normal level of 160 U/L as after operation (Fig. 3).
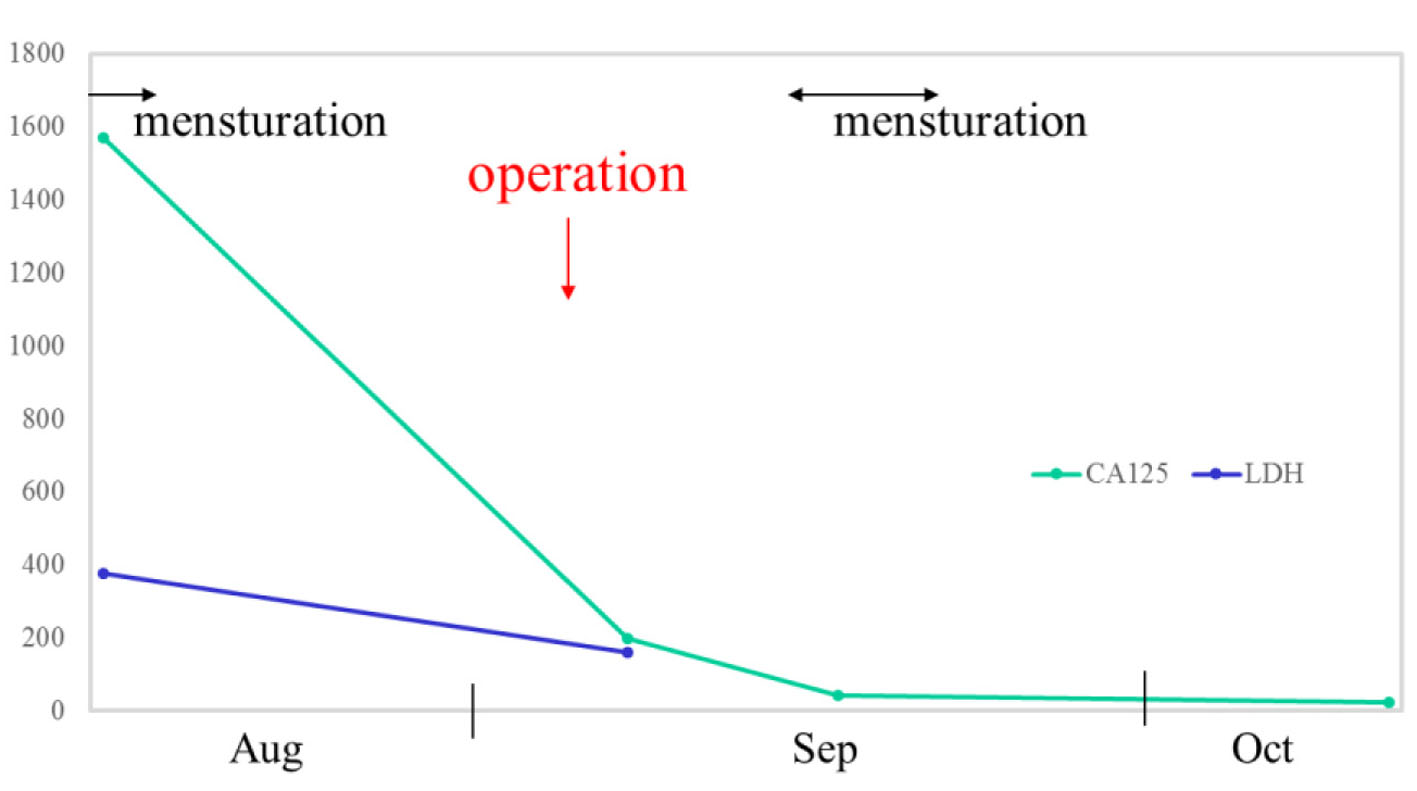 Click for large image | Figure 3. The serum CA125 level (upper, green line) fell from 1,570.9 U/mL at presentation, to 197.2 U/mL 1 day after the operation, to 42.6 U/mL during the next menstruation, and finally to 23.4 U/mL, a normal level, within a month after the operation. A re-elevation of the CA125 level did not occur, even during the next menstruation period after the operation. Immediately after the operation, the serum LDH level (blue line) also dropped. |
| Discussion | ▴Top |
An elevated serum LDH level is often associated with cases of leiomyosarcoma [2]. In a report by Goto et al concerning serum LDH isozymes, both total LDH and LDH isozyme type 3 were elevated [3]. There are no reports that LDH levels are increased during menstruation in leiomyosarcoma, nor in cases of leiomyoma without a degenerative pattern. The reason why her serum LDH level was high before the operation is unknown. The timing of the blood sampling was just after an exercise interval and that may have caused the elevated serum LDH levels [4].
Increased serum CA125 level is associated with ovarian, uterine, breast, pancreas, colon, and lung cancers, also endometriosis, adenomyosis, leiomyoma, benign ovarian tumor, hepatic cirrhosis, pleuritis, pericarditis, peritonitis, ascites retention, early pregnancy, and menstrual period [5-10]. In the present case, the patient had an unusually large leiomyoma and the blood sampling was done during menstruation. Regardless, the serum CA125 level (1,570.9 U/mL) was abnormally high. In the report by Kan et al, the peak level of CA125 during normal menstruation was 51.8 ± 6.5 U/mL [11].
According to a recent view, the rise of serum CA125 level associated with leiomyoma is usually quite small. There are only three reports of patients with leiomyoma accompanied by very high CA125 level (> 1,000 U/mL). In the report by Cho et al, the patient (28 years old) had a subserosal leiomyoma and was in early pregnancy [12]. In the Ghaemmaghami et al’s report, one patient (46 years old) had an intramural leiomyoma and the other patient (16 years old) had multiple leiomyomas and a high CA125 level during the menstrual period [13].
Leiomyomas are not normally closely associated with any specific tumor markers, although a study by Babacan et al found an increase in several tumor markers in association with uterine leiomyomas [14]. An increase in CA125 levels was found in 20% of patients with leiomyoma. The mean CA125 level of the patients was 27.3 ± 38.1 U/mL. They found that the factors related to higher levels of CA125 in patients with leiomyoma were larger size (≥ 5 cm), subserosal location, and co-existence with adenomyosis. Bischof et al also found that large leiomyoma size was strongly associated with higher serum CA125 levels [15]. Indirect effects caused by larger leiomyoma, such as peritoneal irritation, were proposed to be responsible for the CA125 elevation.
On the other hand, in the present case, immunostaining for CA125 showed positive staining of the leiomyoma. This suggests that the leiomyoma was producing the CA125. However, similar immunohistochemical findings for leiomyomas are limited in the literature. Adenomatoid tumors have been found positive for CA125 immunostaining [16]. Uterine adenomatoid tumors are typically a solitary mass located subserosally in the posterior wall near the uterine horn. They are often grossly similar to a leiomyoma. However, an adenomatoid tumor has bundles of smooth muscle fibers and stroma showing the presence of small cystic spaces and clusters of round to oval cells. These histological markers were absent in our case.
The serum CA125 level dropped rapidly, from 1,570.9 U/mL at first consultation to 197.2 U/mL by the day following the operation. Considering that the normal half-life of CA125 in serum is about 5 days [17], the CA125 decline appeared to have occurred far too quickly. We now theorize that the serum CA125 may have been dropping from the initial reading even before the operation. Calculating backwards, the CA125 level may have been about 400 U/mL 5 days before the operation, and may have continued to fall regardless of performing myomectomy.
The reason why the CA125 level might have been spontaneously dropping is unknown. In the present case, the leiomyoma clearly was producing the elevated CA125, although the mechanism of the CA125 production by the tumor is also unexplained. There may have existed a cycle of CA125 that the leiomyoma produced, and the peak may have been during menstruation. The high level of CA125 found at first consultation was well before the operation and was measured during menstruation; we may have incidentally observed the highest level of CA125 produced by the leiomyoma because of that point in the menstrual cycle. After the myomectomy, without the leiomyoma, the serum CA125 level was never elevated again. In the literature, there are very few previous findings of production of CA125 by a leiomyoma. Furthermore, we need further exploration of whether the CA125 that the leiomyoma produces goes up and down in concordance with the menstrual period.
In conclusion, the elevated level of serum CA125 recorded at presentation of this unusual case was shown to be produced by a leiomyoma. It is quite rare that a case of leiomyoma is associated with such a high level of CA125. The elevated CA125 level is presumed to have already begun to drop significantly even before the surgical removal of leiomyoma. The mechanism of this unusual fluctuation of serum CA125 related to the leiomyoma is still unknown, but others should be aware that it does occur.
Acknowledgement
The authors thank Dr. Buzard GS for his editing of the manuscript.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
| References | ▴Top |
- Parker WH. Etiology, symptomatology, and diagnosis of uterine myomas. Fertil Steril. 2007;87(4):725-736.
doi pubmed - Seki K, Hoshihara T, Nagata I. Leiomyosarcoma of the uterus: ultrasonography and serum lactate dehydrogenase level. Gynecol Obstet Invest. 1992;33(2):114-118.
doi pubmed - Goto A, Takeuchi S, Sugimura K, Maruo T. Usefulness of Gd-DTPA contrast-enhanced dynamic MRI and serum determination of LDH and its isozymes in the differential diagnosis of leiomyosarcoma from degenerated leiomyoma of the uterus. Int J Gynecol Cancer. 2002;12(4):354-361.
doi pubmed - Ceci R, Duranti G, Sgro P, Sansone M, Guidetti L, Baldari C, Sabatini S, et al. Effects of tadalafil administration on plasma markers of exercise-induced muscle damage, IL6 and antioxidant status capacity. Eur J Appl Physiol. 2015;115(3):531-539.
doi pubmed - Medeiros LR, Rosa DD, da Rosa MI, Bozzetti MC. Accuracy of CA 125 in the diagnosis of ovarian tumors: a quantitative systematic review. Eur J Obstet Gynecol Reprod Biol. 2009;142(2):99-105.
doi pubmed - Povolotskaya N, Das N, Dhar K, Brinkmann D, Gardner F, Woolas R. Utility of Preoperative CA125 Assay in the Management Planning of Women Diagnosed with Uterine Cancer. Surg Res Pract. 2014;2014:497478.
doi - Zhang SJ, Hu Y, Qian HL, Jiao SC, Liu ZF, Tao HT, Han L. Expression and significance of ER, PR, VEGF, CA15-3, CA125 and CEA in judging the prognosis of breast cancer. Asian Pac J Cancer Prev. 2013;14(6):3937-3940.
doi pubmed - Streppel MM, Vincent A, Mukherjee R, Campbell NR, Chen SH, Konstantopoulos K, Goggins MG, et al. Mucin 16 (cancer antigen 125) expression in human tissues and cell lines and correlation with clinical outcome in adenocarcinomas of the pancreas, esophagus, stomach, and colon. Hum Pathol. 2012;43(10):1755-1763.
doi pubmed - Dai H, Liu J, Liang L, Ban C, Jiang J, Liu Y, Ye Q, et al. Increased lung cancer risk in patients with interstitial lung disease and elevated CEA and CA125 serum tumour markers. Respirology. 2014;19(5):707-713.
doi pubmed - Jacobs I, Bast RC, Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod. 1989;4(1):1-12.
pubmed - Kan YY, Yeh SH, Ng HT, Lou CM. Effect of menstruation on serum CA125 levels. Asia Oceania J Obstet Gynaecol. 1992;18(4):339-343.
doi pubmed - Cho FN, Liu CB, Li JY, Chen SN, Yu KJ. Dramatic changes of CA 125 levels in a pregnant woman with a degenerated subserosal myoma. Taiwan J Obstet Gynecol. 2012;51(1):117-118.
doi pubmed - Ghaemmaghami F, Karimi Zarchi M, Hamedi B. High levels of CA125 (over 1,000 IU/ml) in patients with gynecologic disease and no malignant conditions: three cases and literature review. Arch Gynecol Obstet. 2007;276(5):559-561.
doi pubmed - Babacan A, Kizilaslan C, Gun I, Muhcu M, Mungen E, Atay V. CA 125 and other tumor markers in uterine leiomyomas and their association with lesion characteristics. Int J Clin Exp Med. 2014;7(4):1078-1083.
pubmed - Bischof P, Galfetti MA, Seydoux J, von Hospenthal JU, Campana A. Peripheral CA 125 levels in patients with uterine fibroids. Hum Reprod. 1992;7(1):35-38.
pubmed - Hirakawa T, Tsuneyoshi M, Enjoji M. Adenomatoid tumor of the ovary: an immunohistochemical and ultrastructural study. Jpn J Clin Oncol. 1988;18(2):159-166.
pubmed - Canney PA, Moore M, Wilkinson PM, James RD. Ovarian cancer antigen CA125: a prospective clinical assessment of its role as a tumour marker. Br J Cancer. 1984;50(6):765-769.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.