Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access
Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc
Journal website http://www.jcgo.org
Case Report
Volume 6, Number 2, June 2017, pages 45-48
Bilateral Thyroid-Type Struma Ovarii in a Postmenopausal Patient: A Case Report and Review of Literature
Muhammad Azhara, Khurram Shafiquea, Twisha Ozaa, M.A. Haseeba, Raavi Guptaa, b
aDepartment of Pathology, MSC 37, Downstate Medical Center, State University of New York, 450 Clarkson Avenue, Brooklyn, NY, USA bCorresponding Author: Raavi Gupta, Department of Pathology, MSC 37, Downstate Medical Center, State University of New York, 450 Clarkson Avenue, Brooklyn, NY, USA
Manuscript submitted March 14, 2017, accepted March 30, 2017 Short title: Bilateral Thyroid-Type Struma Ovarii doi: https://doi.org/10.14740/jcgo442w
Struma ovarii is a monodermal variant of a germ cell tumor composed predominantly of thyroid tissue. It is most often unilateral with an incidence of 0.3-0.7%. Bilateral struma ovarii is rather rare with only two cases reported in peri- and postmenopausal patients. Here, we present a third case of bilateral struma ovarii in a postmenopausal female with slowly enlarging pelvic mass and pelvic organ prolapse. The patient was treated with total hysterectomy and bilateral salpingo-oophorectomy which revealed bilaterally enlarged cystically dilated ovaries. Histopathologic examination showed mature thyroid follicles with abundant colloid consistent with bilateral struma ovarii. No teratomatous elements or features of malignancy were identified. Thyroid hormone levels were within their respective reference ranges as was also observed in the previous two cases. A diagnosis of bilateral struma ovarii should be considered in the differential diagnosis of bilateral pelvic masses in peri- and postmenopausal patients. There was no clinical or laboratory evidence of hyperthyroidism in any of the three patients.
Teratomas are germ cell tumors that may be monodermal or polydermal (originating from one or more than one germ cell layers). The germ cell components like hair, bone, muscle, teeth and thyroid can be mature or contain variable amounts of immature elements (typically primitive/embryonal neuroectodermal) prompting mature or immature designation [1, 2]. Struma ovarii is a monodermal variant of ovarian teratoma that contains predominantly or exclusively thyroid tissue [3].
Struma ovarii is a rare gynecological tumor that was first described in 1890s [1]. It has an incidence of 0.3-0.7% among the ovarian tumors in the reproductive age group. Bilateral struma ovarii is predominantly a unilateral tumor with only two previously reported cases [2–4]. Here, we report a rare case of bilateral struma ovarii in a postmenopausal patient.
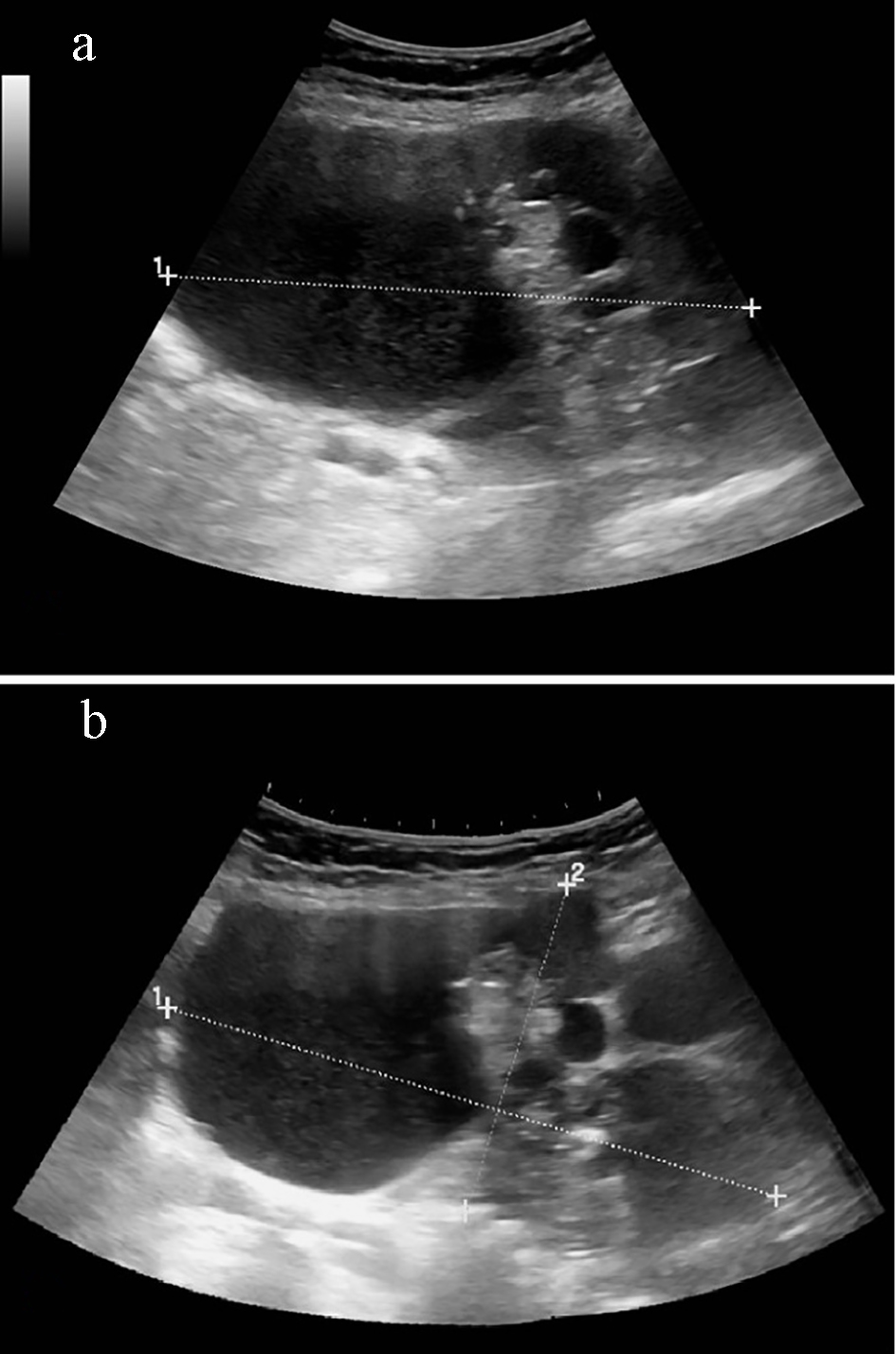
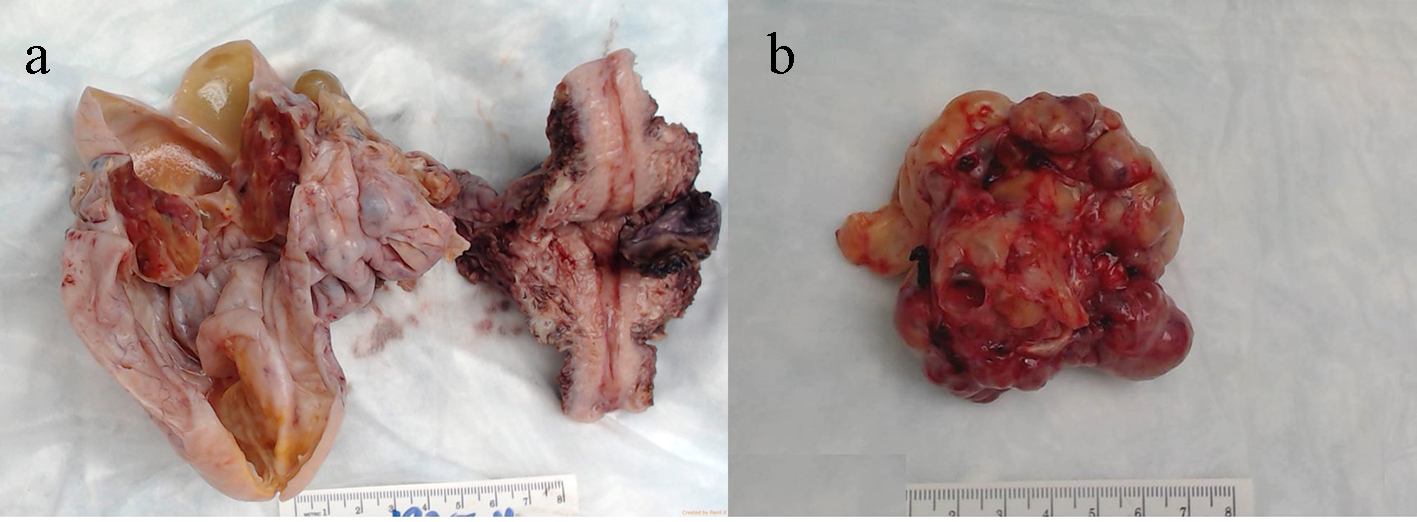
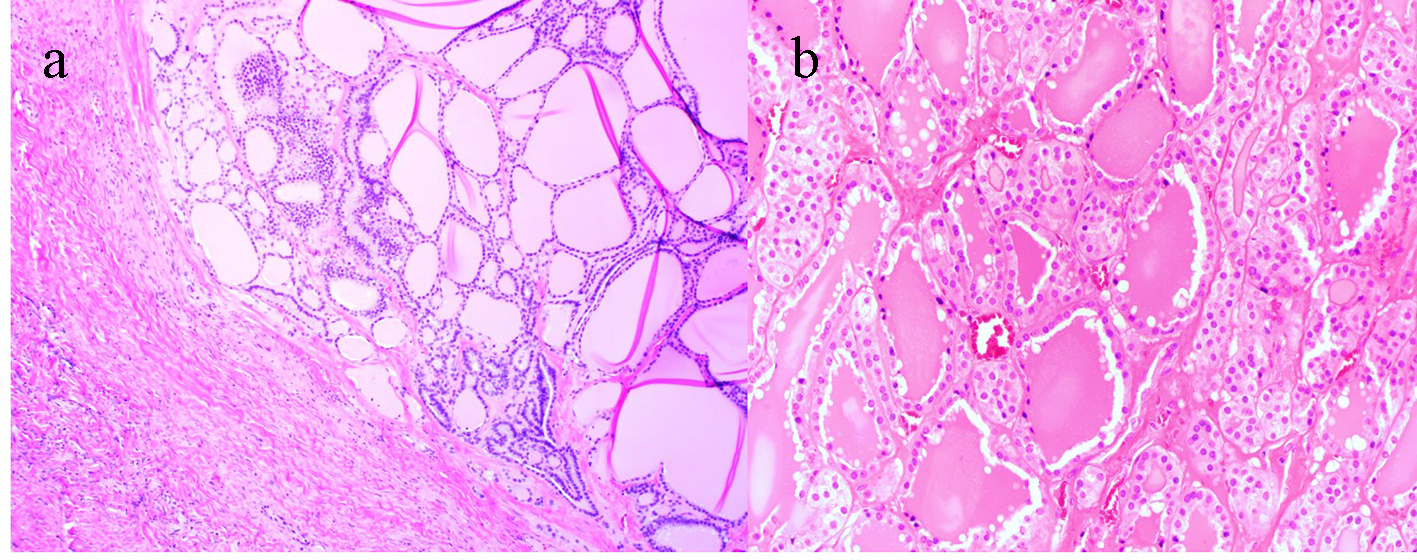
A 64-year-old multiparous female of Caribbean descent was admitted for evaluation of her abdominal distention, shortness of breath, and worsening pelvic organ prolapse. Pelvic examination revealed pelvic organ prolapse and a large pelvic mass. The pelvic mass measured 18.68 × 13.72 × 9.76 cm by ultrasonography (Fig. 1). Routine basic metabolic panel and tumor markers CA125, CA19-9 and carcinoembryonic antigen (CEA) were within the reference ranges. Robot-assisted laparoscopic total hysterectomy, bilateral salpingo-oophorectomy, sacrocolpopexy and Burch suspension were performed. Ovarian cyst was ruptured in situ during the procedure to exclude involvement by an infiltrating tumor. The specimens were delivered via vagina and examined intraoperatively. The uterus with bilaterally enlarged cystically dilated adnexal masses weighed 71 g. Right and left ovarian cysts measured 12 and 8 cm, respectively. Examination of cut surfaces of both cysts showed a complex multicystic mass with focal solid areas (Fig. 2). The cystic areas were filled with serous fluid. Solid areas measuring 3 - 4.2 cm were composed of tan to pink fleshy and spongy tissue, and were sampled extensively. Histopathologic examination of the solid areas in both cysts showed thyroid follicles with abundant colloid and focal areas of calcification. There was no other teratomatous tissue identified (Fig. 3). A diagnosis of bilateral struma ovarii was made. Her postoperative course was uneventful. Postoperatively, T3, T4, TSH, serum thyroglobulin, and CA125 were within their respective reference ranges. Thyroid ultrasonogram was within normal limits.
Figure 1. (a) Complex heterogenous pelvic mass with predominantly cystic and some solid echogenic areas measuring 18.68 × 13.72 × 9.76 cm (transverse view). (b) Mass involves both right and left adnexal regions and extends superiorly into the abdominal cavity (sagittal view).
Struma ovarii is a germ cell ovarian tumor usually seen in the reproductive age group. These tumors are most often unilateral and benign. Only two cases of bilateral struma ovarii have thus far been reported in the literature [3, 4]. Here we present a case of bilateral struma ovarii in a postmenopausal patient and compare our findings with those of the two previous cases.
Of the two previously documented cases with this tumor of the reproductive age group, one was perimenopausal and the other was postmenopausal. Thus, the more common unilateral struma ovarii and the rare bilateral tumor occur in different age groups. Struma ovarii may present as abdominal mass, abdominal pain, abnormal uterine bleeding, pseudo-Meigs’ syndrome (ascites, pleural effusion and ovarian mass), hyperthyroidism and/or as an incidental finding [4, 5]. The presenting symptoms of the three cases with bilateral struma ovarii were abdominal distension, shortness of breath and pelvic organ prolapse caused predominantly by space occupying lesions in the pelvis without any hormonal alteration. Of the two cases that we review here, one presented with pseudo-Meigs’ syndrome and elevated CA125 which normalized following surgical excision of ovarian masses [4]. Cysts ranged in size from 2 to 12 cm. Extensive sampling of the cysts in all three cases did not reveal any features of malignancy.
Both unilateral and bilateral struma ovarii appear as multicystic masses with pink-brown, and spongy tissue with mature thyroid follicles. Malignancies identified in struma ovarii are thyroid-type tumors (papillary, follicular, and highly differentiated follicular carcinoma of ovary), ovarian-type tumors (serous, mucinous, and Brenner’s) or other tumors (carcinoids and malignant melanoma). These malignancies, however, have been reported only in unilateral struma ovarii [6, 7].
Imaging studies (sonography, CT and MRI scans) provide only non-specific information. Triple-contrast CT and iodine-123 scans can be performed to evaluate the extent of disease and whether adjacent structures or lymph nodes are involved.
Patients with struma ovarii rarely have clinical or biochemical evidence of hyperthyroidism despite the abundance of mature thyroid tissue in their ovarian mass. Hyperthyroidism is usually associated with malignant struma ovarii. It may be an incidental finding in the workup of patients with hyperthyroidism with normal-appearing thyroid and abnormal function tests [8, 9]. Thyrotoxicosis may also result from peritoneal strumosis, where mature thyroid tissue implants in the peritoneal cavity [10].
In addition to thyroid function tests, CA125 is a widely used tumor marker for ovarian and other cancers. It is of little significance in struma ovarii as it can be elevated in both benign and malignant tumors, and the degree of elevation does not correlate with malignancy [1]. It is secreted by mesothelial (e.g., peritoneal, pleural, pericardial, and cells) and non-mesothelial (e.g., cervical, endometrial, and amniotic membrane) cells. The mechanism of its elevation may include infiltration of peritoneum by malignant cells, peritoneal stretching by ascites, and low hepatic clearance in cirrhotic patients. Surgical removal of ovarian masses rapidly decreases its levels as observed in one of the two cases from the literature that we have reviewed (Table 1).
Table 1. Summary of Selected Features of Bilateral Struma Ovarii
Surgical resection is the treatment of choice in struma ovarii with postoperative monitoring by iodine-123 scans and measuring serum thyroglobulin [11-13]. In addition, CA125 may be used to monitor recurrence in patients with preoperative CA125 elevations. Postoperatively, disease-free survival for our patient and for one of the two reviewed cases [4] has been recorded to be 2 years.
We have presented a case of bilateral struma ovarii in a postmenopausal woman who came to medical attention for slowly developing pelvic mass and pelvic organ prolapse in the absence of thyroid dysfunction. Bilateral struma ovarii occur in the older postmenopausal patients, and unilateral tumors occur in females of reproductive age. Increased awareness of the occurrence of the distinct age groups these tumors affect is expected to help clinicians include struma ovarii in their differential diagnosis of bilateral ovarian tumors.
Novac L, Niculescu M, Simionescu C, Stanescu MR, Novac M. Bilateral struma ovarii: a case mimicking an ovarian neoplasm. Eur J Gynaecol Oncol. 2008;29(4):414-416. pubmed
Rana V, Srinivas V, Bandyopadhyay S, Ghosh SK, Singh Y. Bilateral benign non functional struma ovarii with Pseudo-Meigs' syndrome. Indian J Pathol Microbiol. 2009;52(1):94-96. doipubmed
Mui MP, Tam KF, Tam FK, Ngan HY. Coexistence of struma ovarii with marked ascites and elevated CA-125 levels: case report and literature review. Arch Gynecol Obstet. 2009;279(5):753-757. doipubmed
Bal A, Mohan H, Singh SB, Sehgal A. Malignant transformation in mature cystic teratoma of the ovary: report of five cases and review of the literature. Arch Gynecol Obstet. 2007;275(3):179-182. doipubmed
Devaney K, Snyder R, Norris HJ, Tavassoli FA. Proliferative and histologically malignant struma ovarii: a clinicopathologic study of 54 cases. Int J Gynecol Pathol. 1993;12(4):333-343. doipubmed
Matsuda K, Maehama T, Kanazawa K. Malignant struma ovarii with thyrotoxicosis. Gynecol Oncol. 2001;82(3):575-577. doipubmed
Zhang X, Axiotis C. Thyroid-type carcinoma of struma ovarii. Arch Pathol Lab Med. 2010;134(5):786-791. pubmed
Wei S, Baloch ZW, LiVolsi VA. Pathology of struma ovarii: a report of 96 cases. Endocr Pathol. 2015;26(4):342-348. doipubmed
Goffredo P, Sawka AM, Pura J, Adam MA, Roman SA, Sosa JA. Malignant struma ovarii: a population-level analysis of a large series of 68 patients. Thyroid. 2015;25(2):211-215. doipubmed
Chan SW, Farrell KE. Metastatic thyroid carcinoma in the presence of struma ovarii. Med J Aust. 2001;175(7):373-374. pubmed
Volpi E, Ferrero A, Nasi PG, Sismondi P. Malignant struma ovarii: a case report of laparoscopic management. Gynecol Oncol. 2003;90(1):191-194. doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.