Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access
Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc
Journal website http://www.jcgo.org
Case Report
Volume 6, Number 2, June 2017, pages 49-52
Serous Endometrial Intraepithelial Carcinoma: Case Report and Literature Review
Mayuko Kawataa, b, Ai Miyoshia, Eri Fujikawaa, Serika Kanaoa, Masumi Takedaa, Mayuko Mimuraa, Masaaki Nagamatsua, Takeshi Yokoia
aDepartment of Obstetrics and Gynecology, Kaizuka City Hospital, Kaizuka, Osaka, Japan bCorresponding Author: Mayuko Kawata, Department of Obstetrics and Gynecology, Kaizuka City Hospital, 3-10-20 Hori Kaizuka, Osaka 597-0015, Japan
Manuscript submitted April 1, 2017, accepted May 19, 2017 Short title: Serous Endometrial Intraepithelial Carcinoma doi: https://doi.org/10.14740/jcgo446w
Serous endometrial intraepithelial carcinoma (SEIC) is a rare but highly aggressive form of uterine endometrial cancer. We present a case of a premenopausal 42-year-old patient who presented with copious vaginal bleeding without a specific medical history. A total abdominal hysterectomy was performed. Pathologic results showed SEIC. We report this case and include a brief literature review.
Today in Japan, endometrial carcinoma (EC) is the most common malignancy of the female genitals. The majority of EC are type 1 estrogen-related tumors of early-stage and low-grade, with a 5-year survival rate of greater than 85% [1].
The second type of EC is the non-estrogen-related type 2 tumors, the most common of which is the serous endometrial adenocarcinoma (SEC). Type 2 EC makes up the preponderance of all EC mortality. Tumor recurrence and death have occurred even when the SEC was thought confined to the endometrium [2, 3].
The serous endometrial intraepithelial carcinoma (SEIC) is limited to the uterine epithelium, but has been shown to be the precursor of invasive SEC. SEIC can be a difficult histopathological diagnosis without ancillary immunohistochemistry [4]. This diagnostic ambiguity is critical because molecular studies have shown that SEIC is commonly the source of extra-uterine metastasis, making it a uniquely aggressive disease [5, 6].
We experienced an unusual case of a premenopausal woman diagnosed with SEIC. We report on this rare case, and provide a brief review of the SEIC literature.
A 42-year-old premenopausal woman (gravida 3) presented to our hospital with copious atypical genital bleeding. She had no previous history of such bleeding or related symptoms. During internal examination, roughly 300 mL of blood with clots was observed in the vagina. Transvaginal ultrasound found no abnormalities in the uterus, endometrium thickness or ovaries. Magnetic resonance imaging (MRI) detected hematometra and an endometrial polyp 13 mm in diameter.
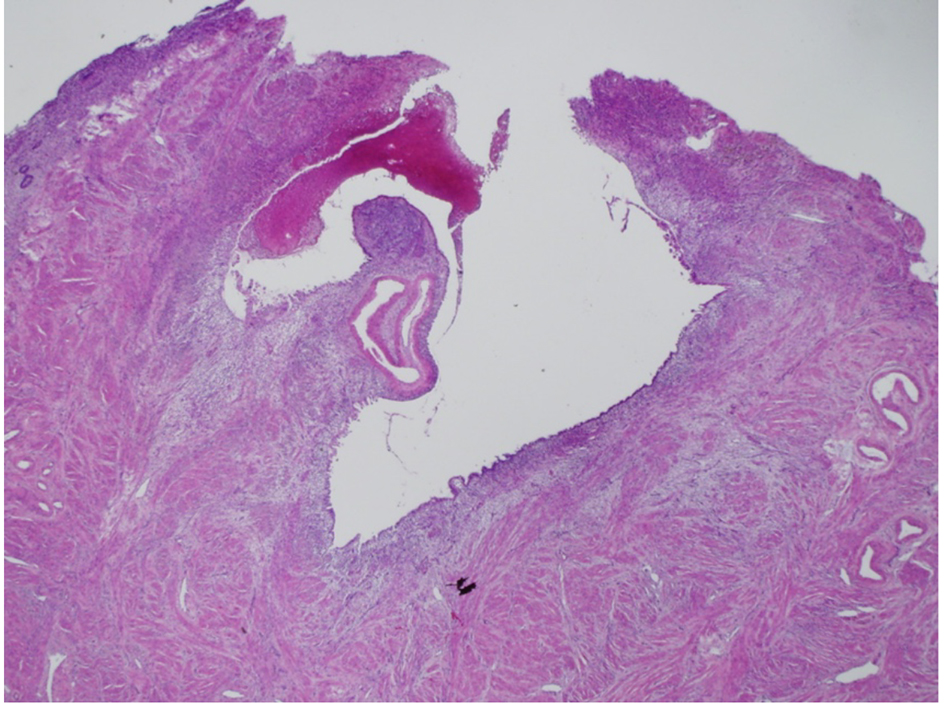
For hemostasis, a total abdominal hysterectomy was performed. The gross appearance of the resected uterus was normal for a 43-year-old female. There was a small round elevated lesion (polyp) arising from the posterior wall of the uterus. The cross-section of the polyp featured a spongiform structure (Fig. 1).
Figure 1. Histological findings of polyp from the posterior uterine wall endometrium. A cystoid tumor spanned the uterine lesion by forming confluent glands (H&E stain; original magnification × 40).
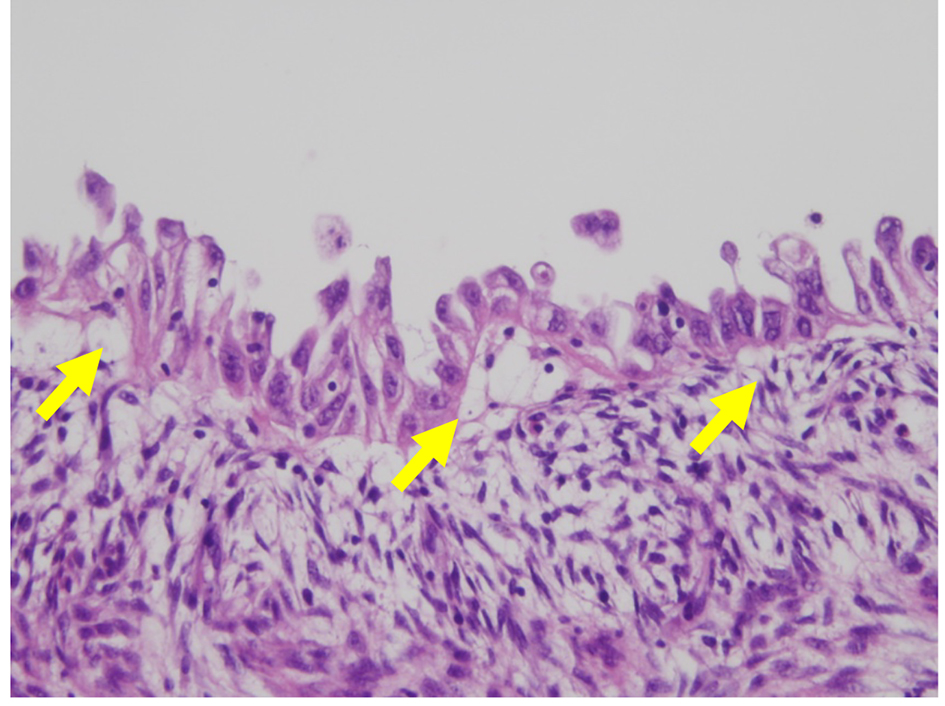
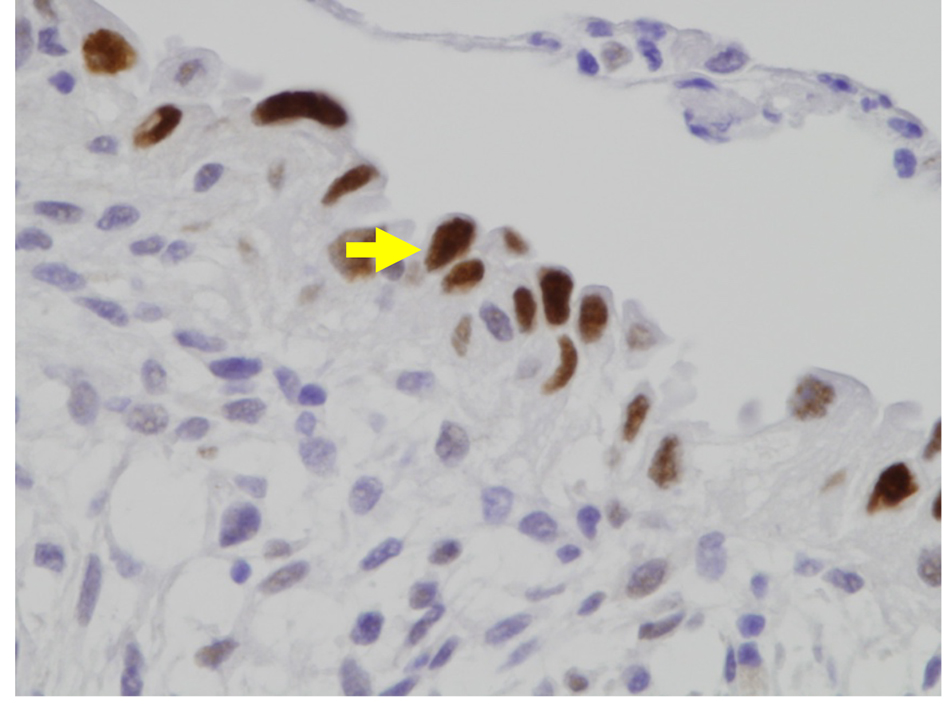
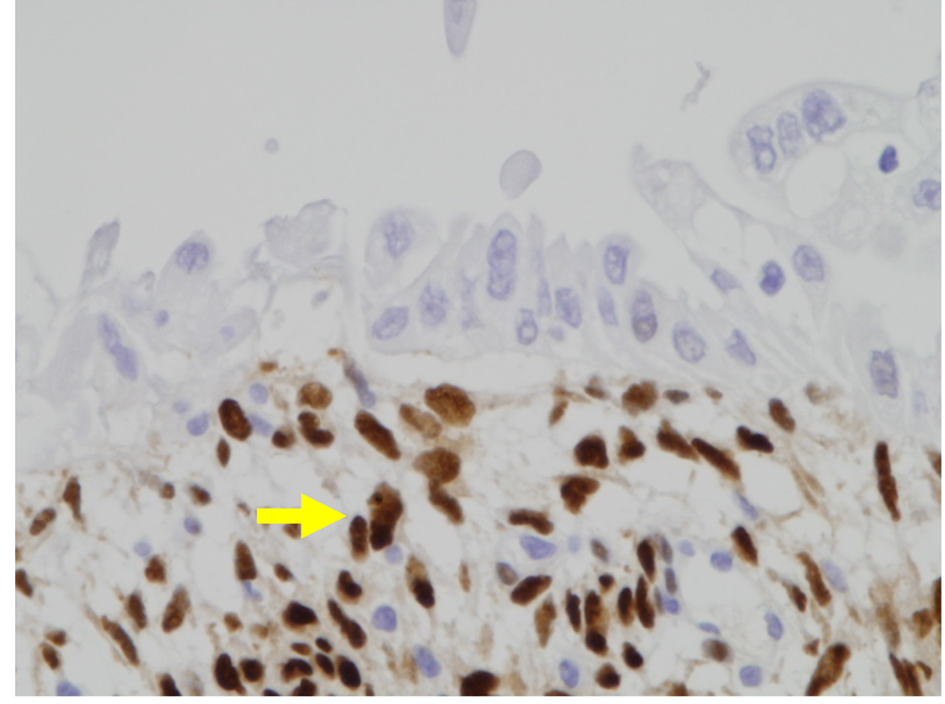
Histologically, cystoid growths spanned the polyp, forming confluent glands measuring 3 - 4 mm in diameter. The tumor cells formed multiple layers and had large nuclei with irregular eosinophilic nucleoli, with a hobnail appearance (Fig. 2). Immunohistochemistry showed that the tumor cells were p53 positive (Fig. 3), estrogen receptor (ER) negative (Fig. 4), and progesterone receptor (PgR) negative (Fig. 5).
Figure 2. Histological findings of the endometrium. The tumor cells formed multiple layers, and had irregular eosinophilic nucleoli, giving the nucleus a hobnail appearance (arrows). The SEIC lesion is limited to the epithelium, showing no stromal invasion. (H&E stain; original magnification × 400).
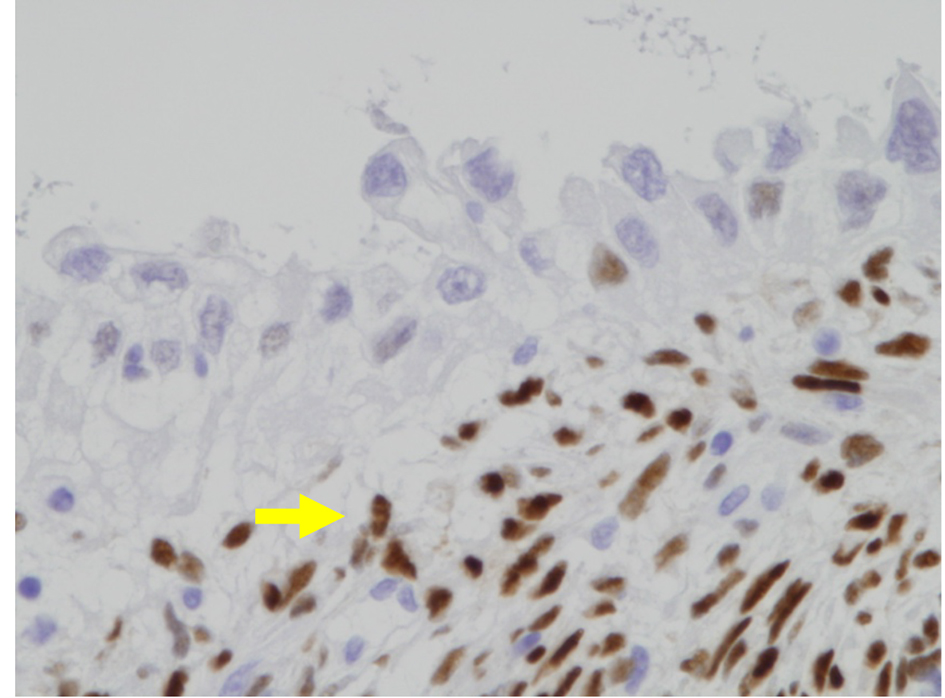
Figure 3. Immunohistochemical findings for the endometrium, showing strongly positive p53 immunostaining in the nucleus of tumor cells (p53; original magnification × 400).
Figure 4. Immunohistochemical findings for the endometrium. Tumor cells have lost estrogen receptor (ER) immunoreactivity (arrow) (ER; original magnification × 400).
Figure 5. Immunohistochemical findings for progesterone receptor (PgR) in SEIC of the endometrium. Malignant cells have lost PgR immunoreactivity (arrow) (PgR; original magnification × 400).
After surgery, computerized tomography (CT) found no metastasis. To detect metastatic lesions, we performed a bilateral salpingo-oophorectomy, partial omentectomy, and pelvic and para aortic lymph node dissections. Histopathological examination found no metastatic lesions in the ovaries, lymph nodes or omentum. The final diagnosis was of an SEIC.
Six cycles of adjuvant chemotherapy with paclitaxel, doxorubicin and carboplatin, given at 3 week intervals, were postoperatively conducted. At 9 months postoperation, there was no sign of recurrence.
Historically, SEIC has been discussed either as an “immediate precursor” or an “early form” of SEC, i.e., the latter infers in situ serous adenocarcinoma, also sometimes called “minimal uterine serous cancer” (MUSC). Regardless of terminology, SEIC is clearly the major SEC precursor, as 100% of SEC that had associated concurrent SEIC had concordant genetic markers (mutations) in both components [7].
SEIC and SEC occur mostly at postmenopausal age, which is one of the characteristics that makes our premenopausal case so remarkably rare. Even when you know to look for it, SEIC is difficult to detect because the lesion is usually focal and small. Occasionally it forms a distinctive polyp. SEIC lesions have atypical endometrial glands with pseudostratification of the lining cells, which are relatively large, with markedly atypical “hobnail” nuclei due to prominent nucleoli.
During progression, SEIC evolves into SEC through multiple molecular pathways [8]. TP53 gene mutations (which appear to be important in the conversion of atrophic endometrium into SEIC) and p53 protein overexpression (p53 signatures) are frequently the earliest hallmarks of SEIC. Immunohistochemical stains for p53 (positive), ER (negative), PgR (negative), and now a number of other markers, can help to identify SEIC and give a differential diagnosis from atypical hyperplasia [9].
Zheng et al reported that SEC arises predominantly in the resting endometrium, manifesting first as p53-immunoreactive, but morphologically normal, endometrial cells, evolving into endometrial glandular dysplasia (EGD) (which is the first morphologically identifiable lesion), then to SEIC, and finally into fully developed invasive SEC [10]. In support, there is often EGD surrounding the SEIC lesion [11]. Spiegel reported that SEIC occasionally involves an endometrial polyp [12], as was seen in our case. The presence of EGD and a polyp are helpful for the diagnosis of SEIC.
Recent studies demonstrate that non-invasive SEIC is equivalent in malignancy prognosis to invasive stage IA SEC. SEIC often shows metastasis, even if the lesion appears limited to the endometrium. Dunton et al reported that surgically identified metastasis is detected in 30-63% of SEIC cases [13]. Goff et al found that the absence of myometrial or lymphovascular space invasions did not accurately predict the presence or absence of extra-uterine metastases [14]. Additional surgical exploration is thus required for all SEIC cases.
Using the presence of concordant genetic markers, tubal serous carcinomas have recently been shown to be largely metastases from SEIC and SEC in the uterus [15]. On the flip side, a tiny minority of uterine SECs arise from primary serous tubal intraepithelial carcinoma (STIC), accounting for the early multifocal SEC disease distribution observed in some patients [16]. SEIC has also been shown to be the metastatic precursor for at least 30% of serous ovarian carcinoma (SOC) [17].
We agree that physicians potentially dealing with SEIC should perform full surgical exploration to detect any metastasis, whenever the preoperative evaluation detects a serous histology in lesions of the endometrium.
We feel that it is good practice to offer endometrium biopsy for postmenopausal women who have atypical genital bleeding. In our case, we could not distinguish between atypical genital bleeding and menstrual bleeding because the patient was not yet postmenopausal. It may be safer to offer an endometrial biopsy to all women with atypical genital bleeding, regardless of menopause status or thickness of the endometrium.
Acknowledgments
The authors thank Dr. GS Buzard for his editing of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest regarding this paper.
Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, Jobsen JJ, Warlam-Rodenhuis CC, De Winter KA, et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet. 2000;355(9213):1404-1411. doi
Sutton GP, Brill L, Michael H, Stehman FB, Ehrlich CE. Malignant papillary lesions of the endometrium. Gynecol Oncol. 1987;27(3):294-304. doi
Hendrickson M, Ross J, Eifel P, Martinez A, Kempson R. Uterine papillary serous carcinoma: a highly malignant form of endometrial adenocarcinoma. Am J Surg Pathol. 1982;6(2):93-108. doipubmed
Robboy SJ. Robboy's pathology of the female reproductive tract. 2nd ed. Edinburgh: Churchill Livingstone/Elsevier; 2009. xxxviii, 1,066 p.
Hui P, Kelly M, O'Malley DM, Tavassoli F, Schwartz PE. Minimal uterine serous carcinoma: a clinicopathological study of 40 cases. Mod Pathol. 2005;18(1):75-82. doipubmed
Wheeler DT, Bell KA, Kurman RJ, Sherman ME. Minimal uterine serous carcinoma: diagnosis and clinicopathologic correlation. Am J Surg Pathol. 2000;24(6):797-806. doipubmed
Kuhn E, Wu RC, Guan B, Wu G, Zhang J, Wang Y, Song L, et al. Identification of molecular pathway aberrations in uterine serous carcinoma by genome-wide analyses. J Natl Cancer Inst. 2012;104(19):1503-1513. doipubmed
Fadare O, Zheng W. Insights into endometrial serous carcinogenesis and progression. Int J Clin Exp Pathol. 2009;2(5):411-432. pubmed
Lax S. [Precursor lesions of endometrial carcinoma: diagnostic approach and molecular pathology]. Pathologe. 2011;32(Suppl 2):255-264. doipubmed
Zheng W, Xiang L, Fadare O, Kong B. A proposed model for endometrial serous carcinogenesis. Am J Surg Pathol. 2011;35(1):e1-e14. doipubmed
Mochizuki S, Marukawa K, Gouda A, Shimizu T, Watanabe R, Onda C. Case report of serous endometrial intraepithelial carcinoma. Hokkaido Bull Jpn Soc Clin Cytol. 2014;23:34-37.
Spiegel GW. Endometrial carcinoma in situ in postmenopausal women. Am J Surg Pathol. 1995;19(4):417-432. doipubmed
Dunton CJ, Balsara G, McFarland M, Hernandez E. Uterine papillary serous carcinoma: a review. Obstet Gynecol Surv. 1991;46(2):97-102. doipubmed
Goff BA, Kato D, Schmidt RA, Ek M, Ferry JA, Muntz HG, Cain JM, et al. Uterine papillary serous carcinoma: patterns of metastatic spread. Gynecol Oncol. 1994;54(3):264-268. doipubmed
Kommoss F, Faruqi A, Gilks CB, Lamshang Leen S, Singh N, Wilkinson N, McCluggage WG. Uterine Serous Carcinomas Frequently Metastasize to the Fallopian Tube and Can Mimic Serous Tubal Intraepithelial Carcinoma. Am J Surg Pathol. 2017;41(2):161-170. doipubmed
Tolcher MC, Swisher EM, Medeiros F, Lima JF, Hilderbrand JL, Donovan JL, Garcia RL, et al. Characterization of precursor lesions in the endometrium and fallopian tube epithelium of early-stage uterine serous carcinoma. Int J Gynecol Pathol. 2015;34(1):57-64. doipubmed
Roelofsen T, van Kempen LC, van der Laak JA, van Ham MA, Bulten J, Massuger LF. Concurrent endometrial intraepithelial carcinoma (EIC) and serous ovarian cancer: can EIC be seen as the precursor lesion? Int J Gynecol Cancer. 2012;22(3):457-464. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.