

| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Original Article
Volume 7, Number 1, March 2018, pages 1-12
Evaluating Women’s Satisfaction With Health Services Received During Childbirth: A Study of Hospitals in Athens, Greece
Pavlos I. Sachsanidis
Department of Health Care Management, School of Social Sciences, Hellenic Open University, Parodos Aristotelous 18, 26335 Patra, Greece
Manuscript submitted January 2, 2018, accepted February 21, 2018
Short title: Health Services During Childbirth
doi: https://doi.org/10.14740/jcgo475w
| Abstract | ▴Top |
Background: Cooperating with healthcare providers during childbirth plays a vital role in women’s satisfaction with their received health services. Therefore, women’s satisfaction with their doctor/midwife during childbirth was assessed and its corresponding factors with the aim of improving health services were identified. The differences concerning users of public and private hospitals were also examined.
Methods: The Kuopio Instrument for Mothers (KIM) (Greek version) questionnaire was used to measure the satisfaction of 139 postpartum women (after either vaginal or cesarean births) who gave birth at either public (n = 97) or private hospitals (n = 42) in the greater Athens area.
Results: Participants’ mean age was 35.5 years; 50.4% were secondary school graduates, 38.1% had higher education, and 11.5% had a postgraduate degree; 83.5% were married; 41.7% worked full-time, 8.6% were unemployed, and 12.2% were housemakers. Almost half (41.7%) had a cesarean section; however, most (86.3%) wished to have had a vaginal birth. Generally, most women were satisfied with the healthcare services provided during childbirth, with more women reporting satisfaction with doctors versus midwives. Moreover, satisfaction was directly correlated with age, past birthing experience, and the information that women received during their pregnancy from the Internet. Women were more satisfied if they had a vaginal delivery rather than a cesarean section. Less educated women were more satisfied with their doctor than their more educated counterparts. Women who gave birth in private, rather than public hospitals, were also more satisfied. Other factors such as family and economic situation, the number of previous births, and a history of miscarriages or abortions did not affect women’s satisfaction.
Conclusions: Most women reported a great desire to express their opinions during childbirth; therefore, hospitals should distribute satisfaction questionnaires to postpartum women before they are discharged. In addition, healthcare providers should improve their communication with women during childbirth, emphasizing necessary information concerning how the birth is progressing. Finally, when they can be done safely, vaginal births should be promoted over cesarean sections. Future research should work to strengthen the knowledge we have about postpartum women’s satisfaction during childbirth.
Keywords: Patients’ satisfaction; Vaginal childbirth; Cesarean section; Postpartum women; Obstetrician; Midwife
| Introduction | ▴Top |
Women have a critical task, both during pregnancy and childbirth. Pregnant women’s contact with health service providers (e.g., midwife, obstetrician-gynecologist (doctor)) occurs over a period of about 9 months and during childbirth. This contact is characterized by both cooperation and trust, and the memory of this relationship will remain with postpartum women forever, leaving them feeling either satisfied or not with their childbirth experience. Therefore, it is imperative to investigate women’s satisfaction with received health services during childbirth.
Purpose
The immediate aim was to evaluate women who gave birth at a hospital in the greater area of Athens, Greece and their satisfaction with the health services they received. The purpose was to determine what aspects of childbirth were and were not adequately addressed by healthcare providers. In addition, differences in women’s demographic data and its relationship with their satisfaction, including comparing users of public and private hospitals, were examined. The goal of this study was to improve the health services provided to women during childbirth.
| Methods | ▴Top |
Study population
This survey was conducted over 3 months in January 2015, in a public and a private hospital in Athens. Information was collected using a questionnaire, which was given personally to each woman who gave birth during the study period at both hospitals.
Inclusion criteria included the following: 1) women’s desire to participate in the survey, 2) being aged older than 18 years, 3) adequate ability to read and write Greek, and 4) gave birth at one of the two study hospitals. Exclusion criteria included the following: 1) the birth of a newborn that ended up either in utero or shortly after birth and 2) the birth of a newborn with severe physical or genetic abnormalities. These women were excluded since it was determined that their emotional state may result in false outcomes.
Procedure
Information was collected between birth and hospital discharge (from the second to sixth day after childbirth). Questionnaires were completed anonymously and confidentially. It was made clear to participants that choosing to complete the questionnaire would not impact their further care or treatment from the hospital staff. The purpose and potential benefits of the research were explained to them, and it was stressed that their participation was voluntary and that they could choose to withdraw from the study at any time.
Questionnaire
The Kuopio Instrument for Mothers (KIM), which was created and validated by Vehvilainen-Julkunen [1], was used to measure women’s satisfaction. It has also been translated and validated in Greek populations [2]. The scale’s reliability is acceptable: Cronbach’s α = 0.85 for 10 questions relating to the physician and Cronbach’s α = 0.94 for 14 questions relating to the midwife. The k-coefficient ranged from 0.325 to 0.924. To use the Greek version, permission from its creators was obtained.
The KIM includes demographic questions relating to postpartum women’s age, basic training, education level, occupation, marital status, the number of prior births, and type of birth (vaginal vs. cesarean section). Then, follow-up questions about prenatal monitoring and women’s opinions were asked and responses were provided using a three-point scale. Next, 10 questions were asked concerning women’s assessment of how they felt towards the physician-obstetrician during delivery, which were answered using a five-point Likert scale (1 - perfectly adequate; 2 - nearly adequate; 3 - almost vulnerable; 4 - totally vulnerable; 5 - I do not remember). Lastly, women assessed cooperation with the midwife during delivery for 14 questions using the same five-point Likert scale.
Statistical analyses
Statistical analyses were conducted using Microsoft Excel 2010 [3] and IBM-SPSS 21 [4]. Initially, the means and standard deviations for quantitative variables were calculated; then, population sub-groups using non-parametric Mann-Whitney (for comparison between two sub-groups) and Kruskal-Wallis (for comparison between more than two sub-groups) methods were compared. The correlations between quantitative variables were evaluated using the non-parametric Spearman correlation coefficient. Lastly, we used the Kolmogorov-Smirnov test to examine the regularity of continuous variables. The significance level was set at P < 0.05.
Ethical considerations
Permission to complete this study was granted from the relevant hospital committees. Questionnaires were completed anonymously.
| Results | ▴Top |
One hundred fifty-two women were recruited; however, 13 did not agree to complete the questionnaire for unknown reasons. Therefore, the data from 139 women were analyzed (effective response rate: 91.44%).
Participants’ demographics and clinical characteristics
Table 1 lists participants’ demographic and clinical characteristics. Participants’ ages ranged from 24 to 46 years.
 Click to view | Table 1. Participants’ Demographic and Clinical Characteristics |
Participants’ education level
All women had attended a secondary school, and most (97.8%) had a high school diploma. Women were further separated into the following three groups: 1) those who had secondary education (i.e., did not have any professional training; e.g., technical school graduate professionals or technical graduate degrees); 2) those who had higher education (i.e., a university degree or degree from a technological educational institute); and 3) those who had a postgraduate degree (e.g., Masters or PhD) (Table 1). Women’s education level and its relationship with hospital type are shown in Figure 1.
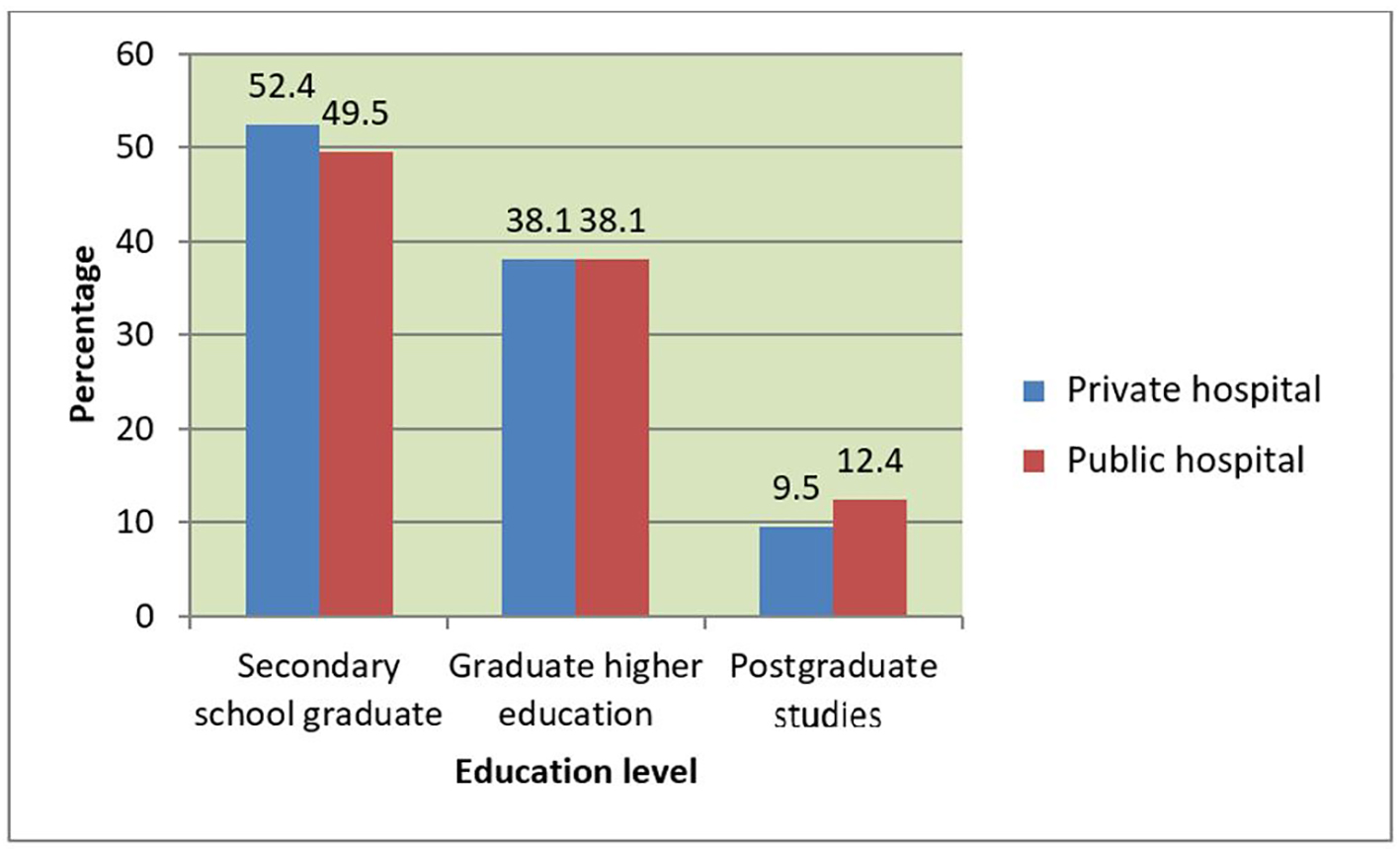 Click for large image | Figure 1. Women’s education level and its association with hospital type (percentage). |
Participants’ marital status and occupation
Participants’ marital status and its relationship with hospital type are shown in Table 2. Participants’ occupations are illustrated in Figure 2.
Click to view | Table 2. Participants’ Marital Status and Its Association With Hospital Type |
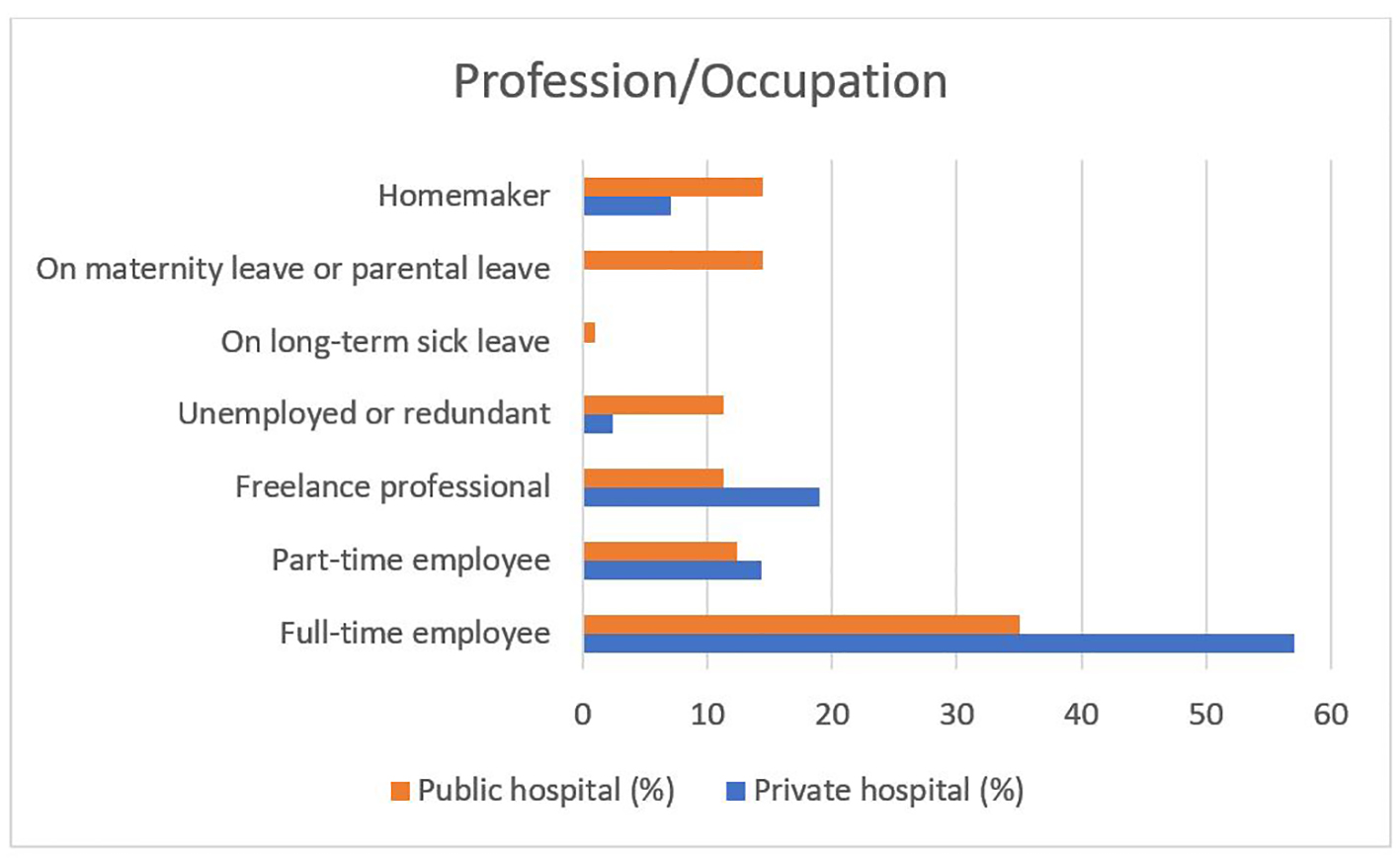 Click for large image | Figure 2. Participants’ professional status (percentage). |
Type of birth
The kind of current childbirth, as well its relationship with hospital type is shown in Table 1. We can also see the women’s preference between vaginal or cesarean section birth.
Description of the birthing experience
Participants’ description of the birthing experience is shown in Figure 3.
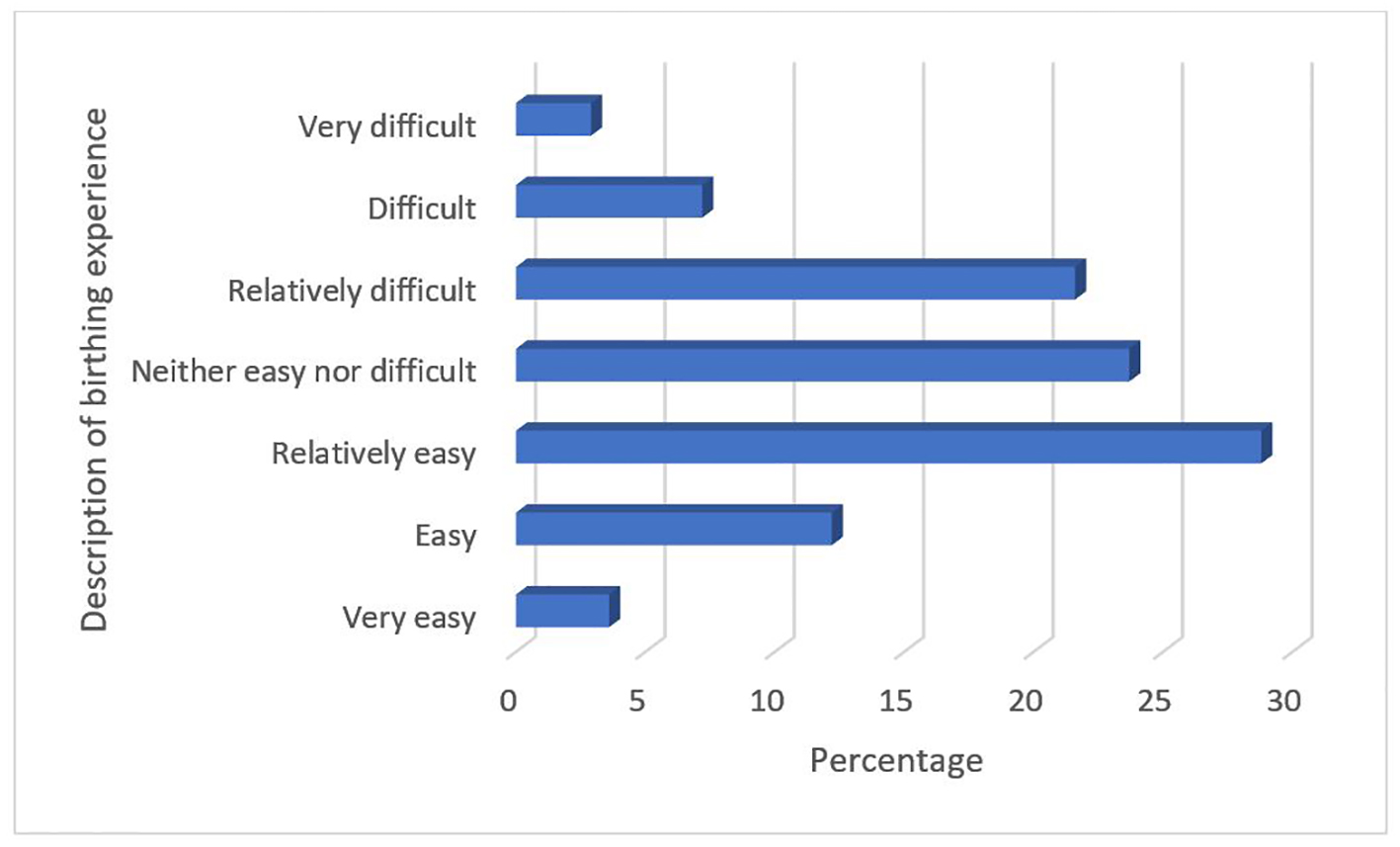 Click for large image | Figure 3. Participants’ description of their birthing experience. |
Public or private hospital
The type of hospital participants gave birth in is shown in Table 1.
Participants’ general satisfaction with childbirth
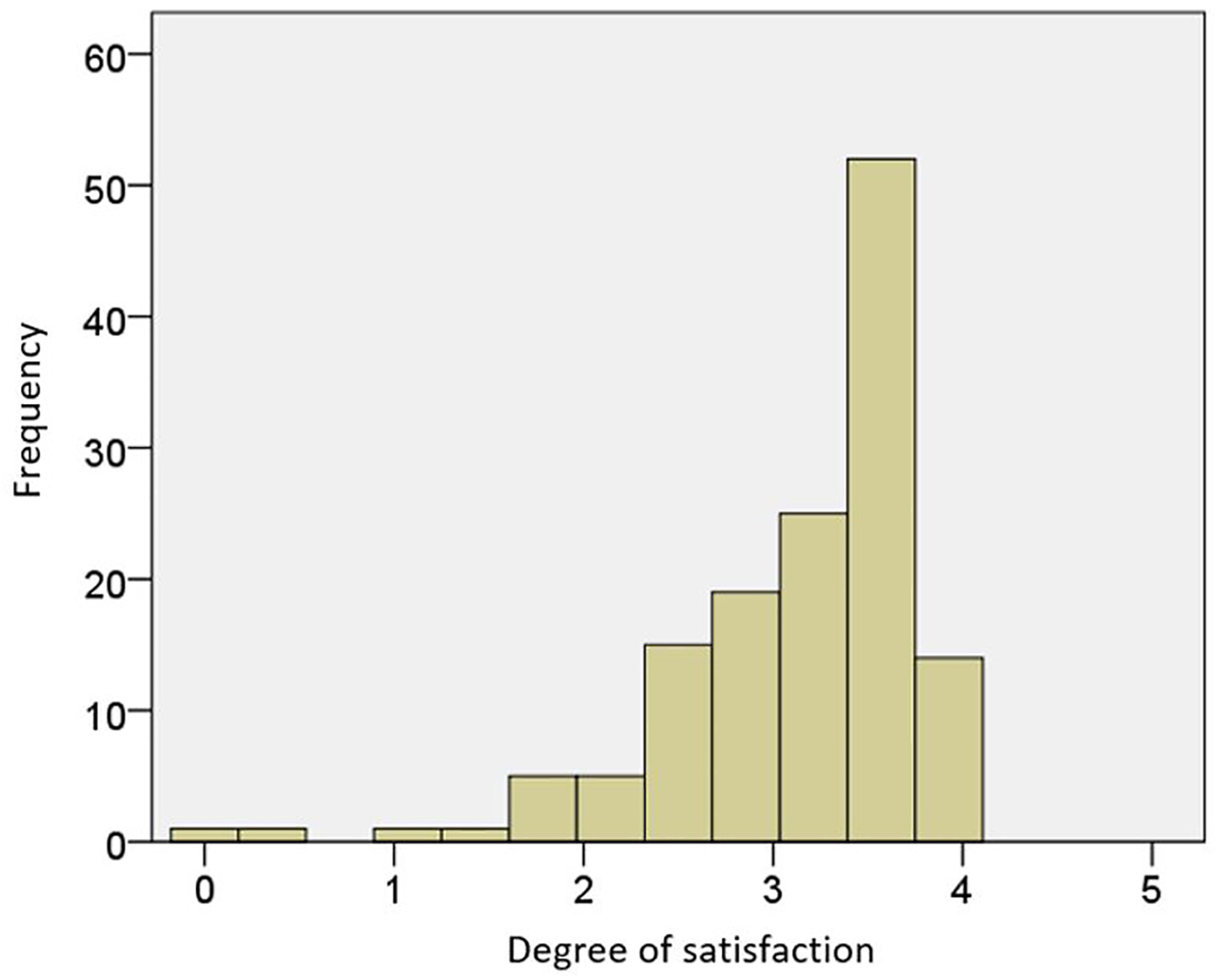
Participants’ satisfaction with the physician and the midwife is shown in Table 3 and Figures 4 and 5 without considering other factors.
Click to view | Table 3. Participants’ Satisfaction With Healthcare Providers During Childbirth |
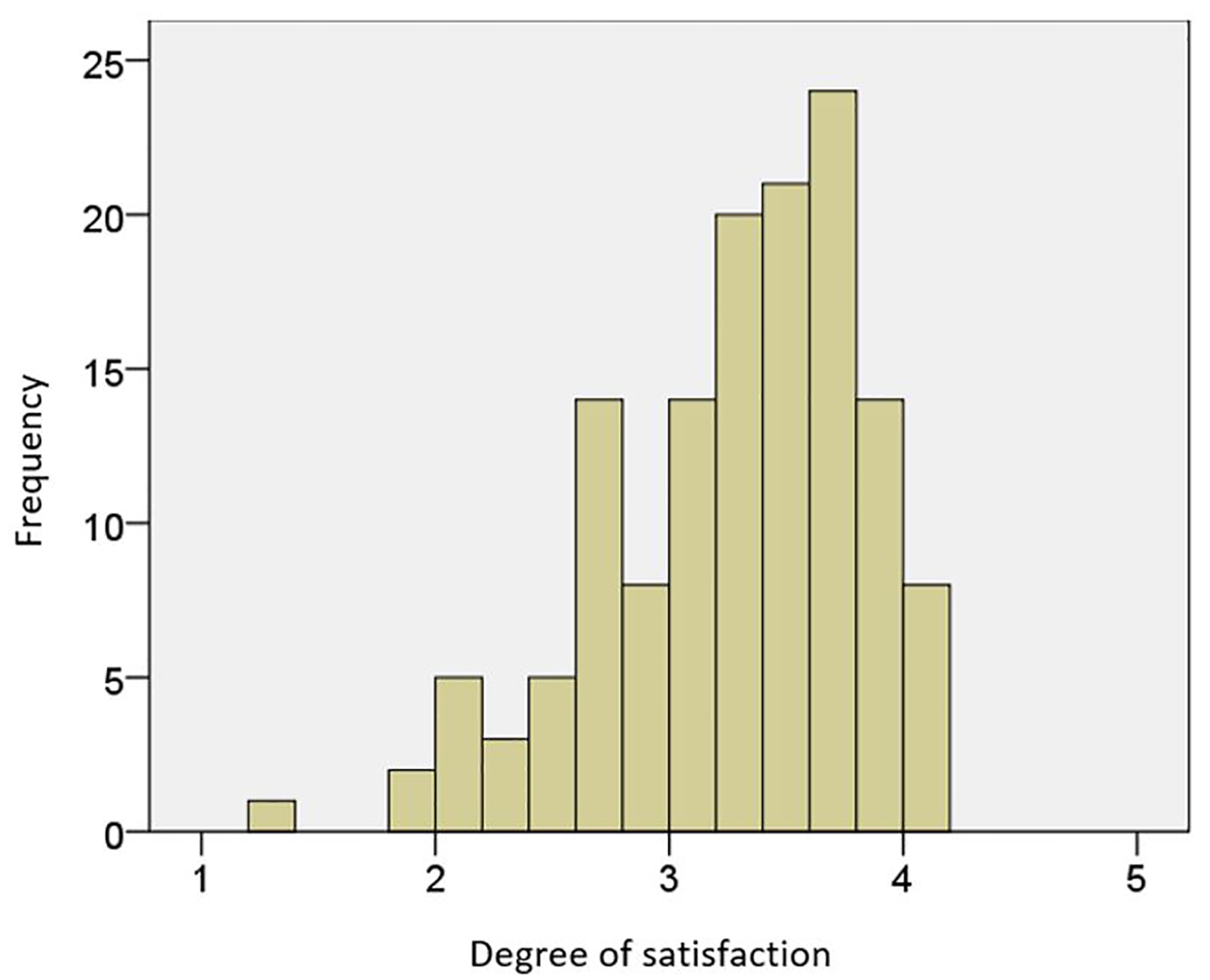 Click for large image | Figure 4. Participants’ satisfaction with their doctor (frequency/degree of satisfaction). |
 Click for large image | Figure 5. Participants’ satisfaction with the midwife (frequency/degree of satisfaction). |
Statistical correlations
During the correlational statistical analyses, a series of descriptive characteristics of the sample were considered. Women’s degree of satisfaction with the doctor and the midwife per these associations were calculated, which are listed below.
Correlation between age and satisfaction with the doctor and the midwife
Participants’ age and its relationship with satisfaction using the non-parametric Kolmogorov-Smirnov test were examined. The distribution of the variables differed significantly (P < 0.05) from the normal distribution; therefore, the non-parametric Spearman correlation coefficient was then used to examine the variables (Table 4).
Click to view | Table 4. Correlation between age and satisfaction with the doctor and the midwife (Spearman correlation coefficient) |
There was a significant negative correlation between women’s age and satisfaction with the healthcare providers. Specifically, the older the women were, the less satisfied they were with their doctor, and vice versa. In contrast, there was no significant relationship between women’s age and satisfaction with the midwives.
Correlation between education level and satisfaction with the doctor and the midwife
There was a significant inverse correlation between education level and satisfaction with the doctor during childbirth. Specifically, the more educated women were, the less satisfied they were with the doctor. These correlations and their relationship per hospital type are shown in Tables 5 and 6.
Click to view | Table 5. Correlation Between Participants’ Education Level and Satisfaction With the Doctor and the Midwife in the Private Hospital |
Click to view | Table 6. Correlation Between Participants’ Education Level and Satisfaction With the Doctor and the Midwife in the Public Hospital |
Correlation between marital status and satisfaction with the doctor and the midwife
Since marital status constitutes a qualitative-categorical variable, if satisfaction with the healthcare providers differentiated between different sub-groups (e.g., single, cohabitating, married, divorced/separated, and widowed) was examined using the non-parametric Kruskal-Wallis test. No significant relationship was observed between women’s marital status and satisfaction with either doctors or midwives.
Correlation between women’s professional status and satisfaction with the doctor and the midwife
No significant relationship was observed between women’s professional status and satisfaction with either doctors or midwives.
Correlation between childbirth history and satisfaction with the doctor and the midwife
No significant relationship was observed between women’s childbirth history and satisfaction with either doctors or midwives.
Correlation between the number of miscarriages or abortions and satisfaction with the doctor and the midwife
There was no significant relationship between the number of miscarriages or abortions and satisfaction with the midwives or doctors during childbirth.
Correlation between childbirth experience and satisfaction with the doctor and the midwife
There was a significant negative correlation between having a negative birthing experience and the degree of satisfaction with the doctor and the midwife (Table 7).
Click to view | Table 7. Correlation Between Participants’ Childbirth Experience and Satisfaction With the Doctor and the Midwife |
Correlation between type of birth and satisfaction with the doctor and the midwife
Women who had a vaginal birth were significantly more satisfied with midwives than were women who had a cesarean section; however, no significant relationship was found regarding birth type and satisfaction with doctors (Figs. 6 and 7).
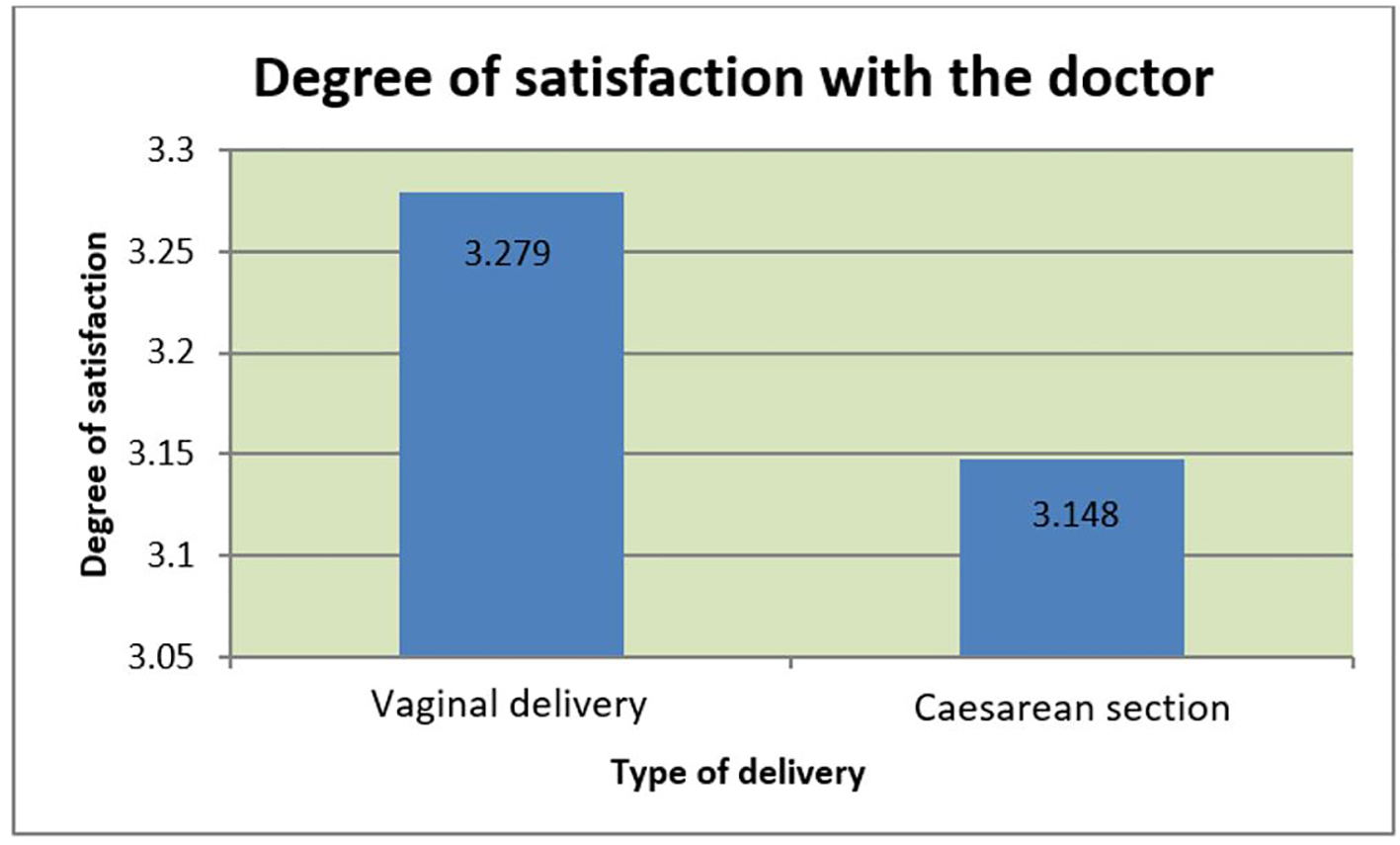 Click for large image | Figure 6. Participants’ satisfaction with the doctor and its association with type of delivery. |
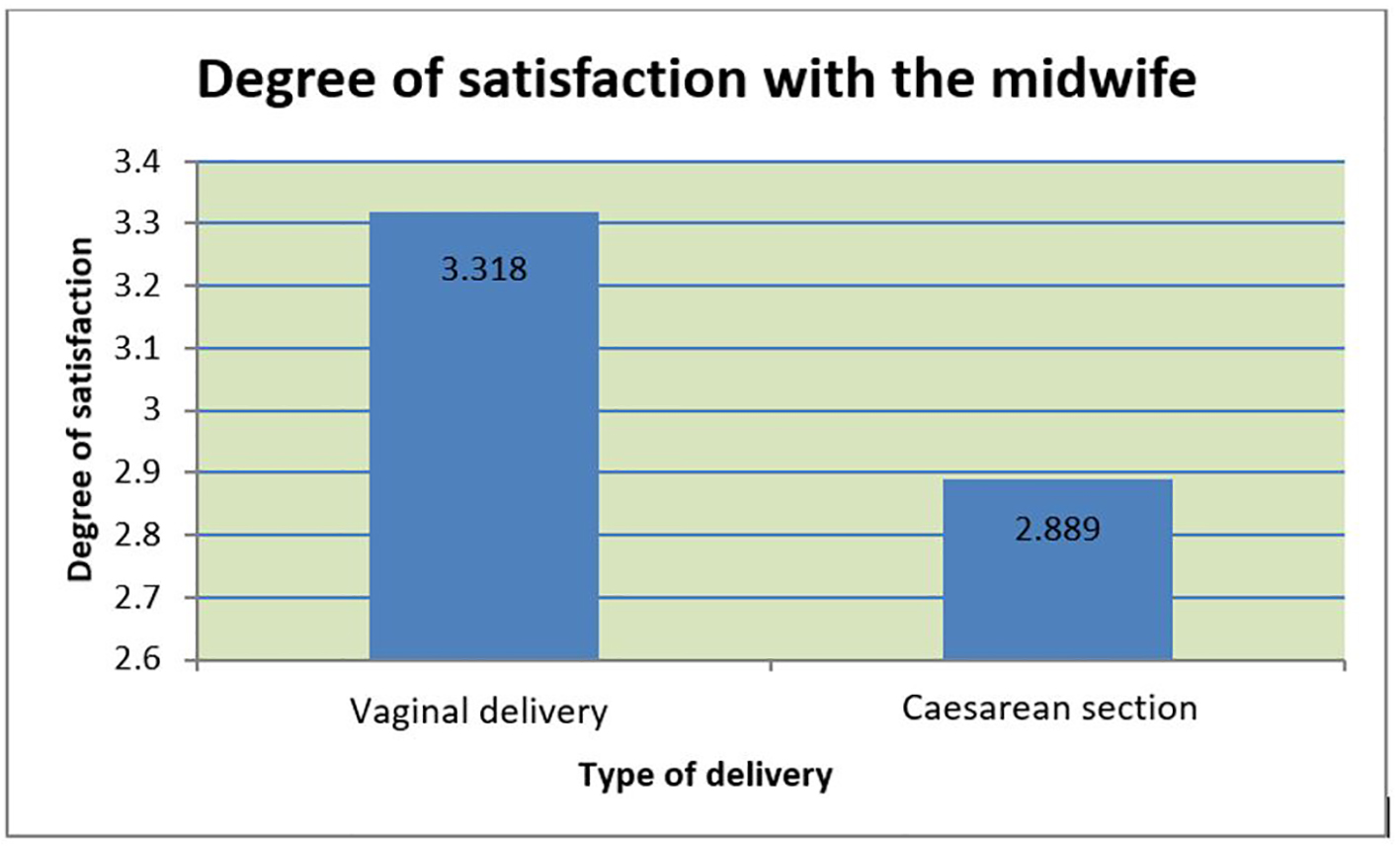 Click for large image | Figure 7. Participants’ satisfaction with the midwife and its association with type of delivery. |
Correlation between the information obtained from the Internet and satisfaction with the doctor and the midwife
Women who obtained information about pregnancy and childbirth from the Internet indicated significantly less satisfaction with both doctors and midwives compared with women who did not obtain information from the Internet (Table 8).
Click to view | Table 8. Correlation Between the Information Participants Obtained From the Internet and Their Satisfaction With the Doctor and the Midwife |
Correlation between utilizing birth preparation courses and satisfaction with the doctor and the midwife
Women who attended birth preparation courses had statistically similar satisfaction levels with their doctor with women who did not attend preparation courses. However, women who attended birth preparation courses tended to be more satisfied than those who did not attend classes. In contrast, the women who attended birth preparation courses were significantly more satisfied with the midwife compared with women who did not attend the courses.
Difference between women’s satisfaction with doctors and midwives per hospital type
Women who gave birth in the private hospital, compared to the public hospital, were significantly more satisfied with both doctors and midwives (Fig. 8).
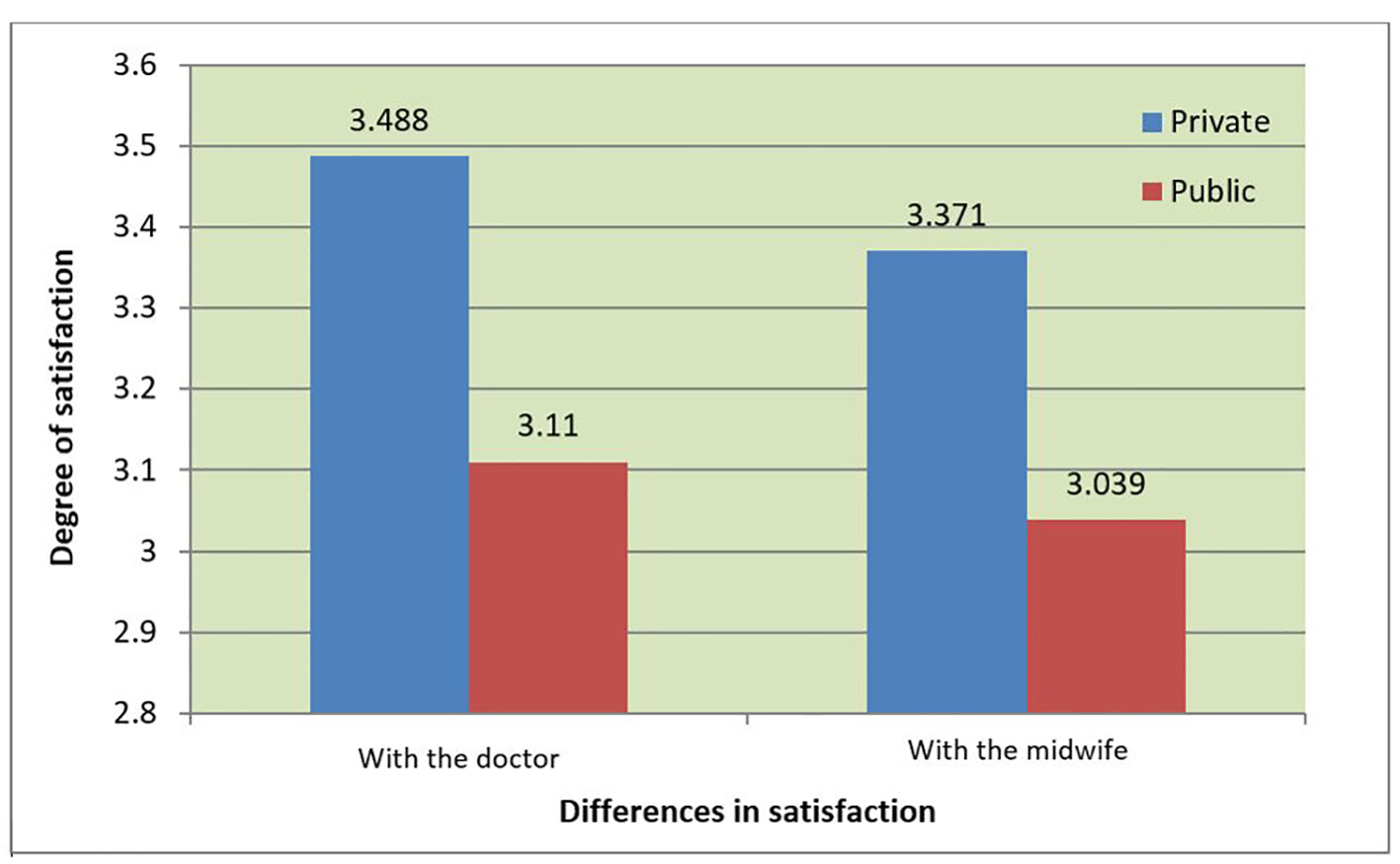 Click for large image | Figure 8. Differences in satisfaction with the doctor and midwife depending on the hospital type. |
| Discussion and conclusion | ▴Top |
Since childbirth is considered a “normal, healthy experience”, pregnant women are not considered as “typical” patients. Consequently, the relationship between pregnant women and healthcare professionals (i.e., doctors and midwives) is critical and should comprise cooperation, friendship, trust, and care. Previous studies have noted that care provided during childbirth has direct effects on the delivery outcome [5-7].
Healthcare providers and healthcare professionals therefore have a vital task in the process of childbirth. Women’s expectations, needs, and experiences should guide the process of both pregnancy and childbirth [8-10]. After giving birth, women should be satisfied not only with the birthing experience, but also with the received health services and the care provided by healthcare professionals. This satisfaction is a multidimensional concept and is associated with many factors, which we measured with a questionnaire.
Women’s mean age in this study (35.5 years) was considered advanced for pregnancy and childbirth. Similar results with women of a mean age of 34 years were found in a survey in northern Greece [11] and in 2010 with women of a mean age of 30 years [12]. Another study with women of a mean age of 29 years [13] showed that women in Greece generally have children at a relatively old age [14].
Regarding women’s education, it was concluded that women with more education were more attracted to the public hospital compared to the private hospital. The fact that many women had obtained higher education and a postgraduate degree might explain the high average age of the childbearing women in this study. This will also be associated with the number of children women have since they may not be fertile for much longer. In addition, women’s professional status was consistent with past surveys where full-time employees were postpartum (23.3%) in northern Greece [12] and public and private employee (38.8% and 32.1%, respectively) in Cyprus [13].
The results indicate that working women and women who are self-employed are likely to have some financial comfort; therefore, they may tend to prefer using the private hospital. Further, unemployed women and homemakers tended to choose to give birth at the public hospital, which is likely associated with the cost of the private hospital.
Consistent with past research in Cyprus [13] and Northern Greece [12], almost all women in this study were married or living with someone. The negligible number of women who gave birth while single is likely due to the conservative attitudes and perceptions toward women and childbirth in Greece [11, 12]. Further analysis of the data showed that about half of the women had not given birth before. This coupled with the statistics regarding women’s age may mean that women plan to only have one child. In addition, contrasting previous results that 38% of postpartum women had had a miscarriage or an abortion [13], results from this study revealed that only 18.7% and 5% of postpartum women had experienced one or two miscarriages or abortions respectively.
Notably, regarding birth type, the clear majority of women preferred to have a vaginal birth rather than a cesarean section. It was also clear that this was associated with women’s satisfaction when their desire was not fulfilled. The rate of cesarean section in this study (41.7%) was relatively high compared with rates established in prior studies in Greece: 33.6% in a 2008 survey [11] and 26.8% in 2010 [12]. However, the rate was consistent with the rate of 40% found in 2014 [13] and 41.6% found in research published in 2005, which was conducted in three Greek hospitals in 2002 [15]. In other words, Greece has a very high rate of cesarean sections.
The high rate of cesarean sections in the greater Athens area raises many questions. One could argue that there are other unstated reasons or motives, apart from noted medical reasons, that contribute to the excessive increase in cesarean sections [16-18]. Many studies have claimed that women prefer to give birth by cesarean section because they are afraid of the pain of vaginal childbirth [19-23]. This, however, does not seem to be the case in this study, since most women wished to have a vaginal birth (Table 1).
Women’s satisfaction with having a vaginal birth might be associated with the fact that cesarean sections are an unpleasant experience and are considered a surgery; therefore, they may be associated with negative experiences. However, research in Germany did not find that cesarean sections were associated with women’s satisfaction during birth [24].
It is also worth mentioning that an increased apprehension about the possible legal proceedings against health professionals in the event of complications during vaginal childbirth may affect the increase in the rate of cesarean sections [12]. Additionally, other factors such as being able to schedule a cesarean section and having the baby faster with a cesarean section compared to vaginal delivery may be associated with doctors preferring, and thus promoting, cesarean sections. In addition, the eclectic selection of women from the doctor and economic benefits may be associated with doctors preferring cesarean sections over vaginal births.
The difference in the rate of cesarean sections between the private and the public hospital could be interpreted by the fact that women chose to go to a private hospital to fulfill their desire to have a vaginal birth. On the other hand, the fact that cesarean sections save the doctor time and the lack of money motivation (since they are paid with a fixed monthly income) may explain the high rate of cesarean sections in the public hospital.
In addition, it is critical to determine women’s opinions of their childbirth experience. In this study, most women reported the experience as “relatively easy” or “neither easy nor difficult”. Only about 10% reported the birth as “difficult” or “very difficult”, implying that the experience was a positive one for most women. These results are encouraging and consistent with other investigations abroad [25]. Specifically, women showed slightly more satisfaction with doctors compared to midwives, which coincides with another survey conducted in northern Greece [12]. This result is consistent with the biomedical model of childbirth [2, 26], which involves the involvement and supervision of the obstetrician-gynecologist [15]. This could also be because many women have the same doctor over the course of their pregnancy, which fosters trust and continuity. On the other hand, women may not meet the midwife until during childbirth, which restricts their relationship. These potential associations have been noted previously [27-31]. It should also be stated that women reported satisfaction when doctors respected their bodies and provided information about the type of birth they were going to have. Furthermore, contrasting results have also been found in Cyprus and abroad, as some studies have noted that postpartum women reported more satisfaction with midwives as opposed to doctors [13, 30, 32-34]. Regardless, both doctors and midwives play a vital role in women’s satisfaction with the birthing process.
Women’s satisfaction with the doctor was associated with receiving an explanation about the use of certain devices and tools and whether they could participate in decisions regarding the birth. This was also observed in other international studies [24, 35, 36]. Moreover, women’s satisfaction with the midwife was associated with whether they could plan the birth along with the midwife including debating possible alternatives and their consequences.
Age was correlated with women’s satisfaction with their doctor. Younger women reported more satisfaction and cooperation with their doctor than did older women; however, no correlation was observed between age and satisfaction with the midwives during delivery. In addition, women’s professional status and past birth experiences were not associated with satisfaction with the healthcare providers.
Regarding education and hospital type, the more educated women were, the less satisfied they were with their doctor, especially when they gave birth at the private hospital; however, this relationship did not exist for midwives or when women gave birth at the public hospital.
Regarding obtained information, women who sought information from the Internet were less satisfied, both with the doctor and the midwife. These results, however, are not consistent with other international research, which noted a positive effect of Internet information on women’s satisfaction [37, 38]. In addition, women who attended some courses to prepare for childbirth reported greater satisfaction with the midwife (and to a lesser extent the doctor) than did women who did not attend these courses.
Finally, women reported greater satisfaction with both doctors and midwives if they gave birth at the private rather than the public hospital. Possible reasons for this could be the smaller percentage of cesarean sections in the private rather than public hospital, which we have revealed as being connected to women’s satisfaction with the birthing experience.
Study limitations
This study had some limitations. First, we only examined hospitals in the greater Athens area. Additionally, the sample of women who participated was negligible compared to the population of all women who give birth in Athens. Lastly, the sample comprised the urban population of Greece; therefore, the results cannot be generalized to the whole country.
Policy proposals
The current results are of vital importance to both doctors and midwives who should always seek to improve the health services they provide during childbirth. In addition, when vaginal birth can be performed safely, it would be wise to reduce the number of cesarean sections to improve women’s satisfaction with the birthing process.
In addition, additional health services should be provided to women during pregnancy, such as providing psychological support and offering courses in psycho-prophylaxis. Women should also be provided with issues related to childbirth through leaflets and brochures. Furthermore, future research should ensure women remain anonymous and the information they offer is treated as confidential, which could enhance the validity of the results. These measures, coupled with cooperation between women, doctors, and midwives, may positively affect women’s postpartum satisfaction with their healthcare providers and toward the birthing process.
| References | ▴Top |
- Vehvilainen-Julkunen K. Family training: supporting mothers and fathers in the transition to parenthood. J Adv Nurs. 1995;22(4):731-737.
doi pubmed - Sapountzi-Krepia D. Maternity care in Greece. Nossileftiki. 2006;45:160-168.
- Microsoft Office | Productivity Tools for Home & Office. [Online]. Available: https://products.office.com/en-us/home. [Accessed: 02-Nov-2016].
- IBM SPSS Statistics - Deutschland. [Online]. Available: https://www.ibm.com/de-de/marketplace/spss-statistics?&cm_mmca1=000024OR&cm_mmca2=10006046&cm_mmc=Search_Google-_-Data%20Science_Data%20Science-_-EP_DE-_-ibm%20spss_Phrase_AW. [Accessed: 02-Nov-2014].
- Delvaux T, Buekens P, Godin I, Boutsen M. Barriers to prenatal care in Europe. Am J Prev Med. 2001;21(1):52-59.
doi - McQuide PA, Delvaux T, Buekens P. Prenatal care incentives in Europe. Study Group on Barriers and Incentives to Prenatal Care in Europe. J Public Health Policy. 1998;19(3):331-349.
doi pubmed - Miller CA. Maternal and infant care: comparisons between Western Europe and the United States. Int J Health Serv. 1993;23(4):655-664.
doi pubmed - Gibbins J, Thomson AM. Women’s expectations and experiences of childbirth. Midwifery. 2001;17(4):302-313.
doi pubmed - Hall SM, Holloway IM. Staying in control: women’s experiences of labour in water. Midwifery. 1998;14(1):30-36.
doi - Parratt J. The impact of childbirth experiences on women’s sense of self: a review of the literature. Aust J Midwifery. 2002;15(4):10-16.
doi - Sapountzi-Krepia D. ‘Greek mothers’ perceptions of their cooperation with the obstetrician and the midwife in the delivery room. Int J Caring Sci. 2008;1(3):124-131.
- Sapountzi-Krepia D. ‘New mothers’ perceptions regarding maternity care services provided in a prefecture of Nothern Greece. Int J Caring Sci. 2010;3(3):129-135.
- Stylianides Con. Evaluation of the health care in obstetrics in Cyprus during the gestation and delivery. Hell Med Arch. 2014;31(3):327-335.
- The World Factbook - Central Intelligence Agency. [Online]. Available: https://www.cia.gov/library/publications/the-world-factbook/geos/gr.html. [Accessed: 01-Nov-2016].
- Mossialos E, Allin S, Karras K, Davaki K. An investigation of Caesarean sections in three Greek hospitals: the impact of financial incentives and convenience. Eur J Public Health. 2005;15(3):288-295.
doi pubmed - Tang S, Li X, Wu Z. Rising cesarean delivery rate in primiparous women in urban China: evidence from three nationwide household health surveys. Am J Obstet Gynecol. 2006;195(6):1527-1532.
doi pubmed - Wax JR, Cartin A, Pinette MG, Blackstone J. Patient choice cesarean: an evidence-based review. Obstet Gynecol Surv. 2004;59(8):601-616.
doi pubmed - WHO | Factors influencing rising caesarean section rates in China between 1988 and 2008, WHO. [Online]. Available: http://www.who.int/bulletin/volumes/90/1/11-090399/en/. [Accessed: 02-Nov-2016].
- Atiba EO, Adeghe AJ, Murphy PJ, Felmingham JE, Scott GI. Patients’ expectation and caesarean section rate. Lancet. 1993;341(8839):246.
doi - Jackson NV, Irvine LM. The influence of maternal request on the elective caesarean section rate. J Obstet Gynaecol. 1998;18(2):115-119.
doi pubmed - Lee LY, Holroyd E, Ng CY. Exploring factors influencing Chinese women’s decision to have elective caesarean surgery. Midwifery. 2001;17(4):314-322.
doi pubmed - Simkin P. The experience of maternity in a woman’s life. J Obstet Gynecol Neonatal Nurs. 1996;25(3):247-252.
doi pubmed - Wiklund I, Edman G, Andolf E. Cesarean section on maternal request: reasons for the request, self-estimated health, expectations, experience of birth and signs of depression among first-time mothers. Acta Obstet Gynecol Scand. 2007;86(4):451-456.
doi pubmed - Spaich S, Welzel G, Berlit S, Temerinac D, Tuschy B, Sutterlin M, Kehl S. Mode of delivery and its influence on women’s satisfaction with childbirth. Eur J Obstet Gynecol Reprod Biol. 2013;170(2):401-406.
doi pubmed - Andrissi L, Petraglia F, Giuliani A, Severi FM, Angioni S, Valensise H, Vannuccini S, et al. The influence of doctor-patient and midwife-patient relationship in quality care perception of italian pregnant women: an exploratory study. PLoS One. 2015;10(4):e0124353.
doi pubmed - Nusbaum J. Childbirth in modern Athens: the transition from homebirth to hospital birth. Penn Bioeth J. 2006;2(2):33-37.
pubmed - Biro MA, Waldenstrom U, Brown S, Pannifex JH. Satisfaction with team midwifery care for low- and high-risk women: a randomized controlled trial. Birth. 2003;30(1):1-10.
doi pubmed - Green JM, Renfrew MJ, Curtis PA. Continuity of carer: what matters to women? A review of the evidence. Midwifery. 2000;16(3):186-196.
doi pubmed - Homer CS, Davis GK, Cooke M, Barclay LM. Women’s experiences of continuity of midwifery care in a randomised controlled trial in Australia. Midwifery. 2002;18(2):102-112.
doi pubmed - Hundley VA, Milne JM, Glazener CM, Mollison J. Satisfaction and the three C’s: continuity, choice and control. Women’s views from a randomised controlled trial of midwife-led care. Br J Obstet Gynaecol. 1997;104(11):1273-1280.
doi pubmed - Johanson R, Newburn M, Macfarlane A. Has the medicalisation of childbirth gone too far? BMJ. 2002;324(7342):892-895.
doi pubmed - Galotti KM, Pierce B, Reimer RL, Luckner AE. Midwife or doctor: a study of pregnant women making delivery decisions. J Midwifery Womens Health. 2000;45(4):320-329.
doi - Harvey S, Rach D, Stainton MC, Jarrell J, Brant R. Evaluation of satisfaction with midwifery care. Midwifery. 2002;18(4):260-267.
doi pubmed - Spurgeon P, Hicks C, Barwell F. Antenatal, delivery and postnatal comparisons of maternal satisfaction with two pilot Changing Childbirth schemes compared with a traditional model of care. Midwifery. 2001;17(2):123-132.
doi pubmed - Blix-Lindstrom S, Christensson K, Johansson E. Women’s satisfaction with decision-making related to augmentation of labour. Midwifery. 2004;20(1):104-112.
doi pubmed - Morgan M, Fenwick N, McKenzie C, Wolfe CD. Quality of midwifery led care: assessing the effects of different models of continuity for women’s satisfaction. Qual Health Care. 1998;7(2):77-82.
doi pubmed - Hildingsson I, Radestad I. Swedish women’s satisfaction with medical and emotional aspects of antenatal care. J Adv Nurs. 2005;52(3):239-249.
doi pubmed - Novick G. Women’s experience of prenatal care: an integrative review. J Midwifery Womens Health. 2009;54(3):226-237.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.